A device capable of autonomous pH sensing and wireless transmitting of the pH value was successfully constructed, as shown in Figure 8. The constructed device is a miniature model; it weighs 1.2 g and has a volume of 0.6 cm3. The approximate dimensions are 18 mm x 8.5 mm x 4.5 mm. As shown in Figure 15, Figure 16, and Figure 17, it can be implanted to the proximity of the lower esophageal sphincter with a single hemostatic clip; no special accessories are needed. A detailed view of a dissected esophagus with the sensor implanted is shown in Figure 19.
The passive rectenna receiver has an overall footprint of only 22 mm2 even though it is optimized for hand-soldering. When the passive rectenna receiver is put into proximity of the pH sensing device (10 cm) when in an active state (24 h after insertion of batteries until full discharge of the batteries), clear voltage spikes can be observed when the device is transmitting. This is shown in Figure 13. The first two short (75 ms) pulses are synchronization pulses. The distance between the end of the second pulse and the beginning of the third pulse is proportional to the Vgs voltage of the ISFET subtracted by 800 mV (100 ms = 900 mV, 200 ms = 1000 mV, etc.). This voltage linearly translates to the pH of the environment that the sensor is subjected to.
Based on a simple two-point calibration with pH buffers of pH 4 and pH 10 (Table 1), the sensor can return stable and repeatable pH value readings (Table 2). A total of four different solutions with known pH were used-pH 0.6 (160 mM solution of hydrochloric acid in the water, mimicking the stomach acid20) and calibration buffers with pH 4, pH 7, and pH 10. The mean error pH values of the sensor were 0.25 and 0.31 when tested in solutions in beakers and an ex vivo model, respectively. The standard deviations of the errors were 0.30 and 0.36, respectively.
When in the proximity of the transmitter (10 cm), the passive rectenna produces a signal with an amplitude of at least tens of millivolts which can be easily detected by a simple comparator or amplified with an ultra-low-power quiescent current operational amplifier. The effect of a mobile phone antenna with an active GSM call has only a minor negative effect on receiving the data from the sensor, as demonstrated in Figure 14. The mobile phone transmission peaks can be filtered by a simple passive RC/LC (resistor-capacitor/inductor-capacitor) filter as they form a high-frequency part of the signal (their frequency is generally above 500 Hz).
In one of the devices, a short circuit between all three of the ISFET electrodes was intentionally made to show how the device's behavior changes when the device is incorrectly assembled. In this case, no voltage-pH response is observed, and the gate voltage is equal to the drain voltage, which is the battery pack voltage (2-3.2 V). The AD converter, which is referenced to an internal 2.048 V reference, then returns the highest possible value, which translates to 2048 mV. Noise may cause slight fluctuations in the ADC output.
Two variants of firmware that can be programmed to the device were developed and tested. The first one (firmware_10s.zip) is intended for short-term experiments where the pH value is transmitted every 10 s. This provides more data points for the cost of reduced battery life, which is limited to around 24-30 h. The other one (firmware_1min.zip) is intended for long-term experiments. The pH value is transmitted once per min. The lifetime of the sensor with a lower sampling frequency is around 5-6 days. There is also a version of the firmware (firmware-test.zip), which does not include the 24 h delay. This file can be used for testing the correct functionality of the electronics before encapsulation. Alternatively, the delay can be modified by changing the code and recompiling the project. The delay was implemented to allow for a full cure of the epoxy or a possibility when the device is manufactured at a different site than the endoscopic surgery room. With the introduced delay, the useful operating life of the device is maximized.
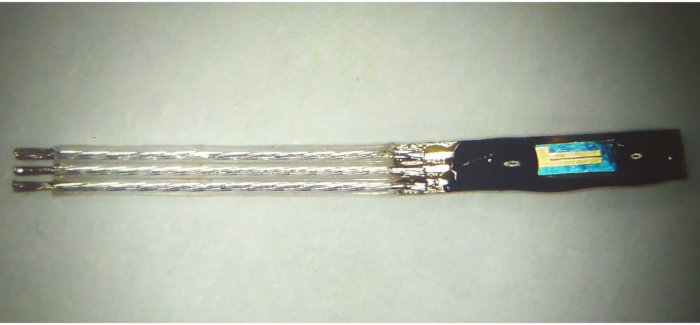
Figure 1: pH sensor assembly before final trimming Please click here to view a larger version of this figure.
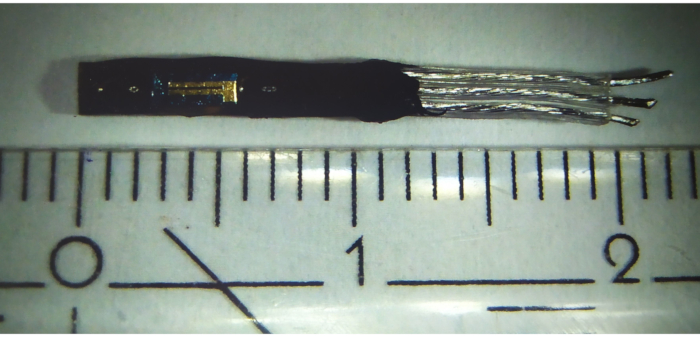
Figure 2: pH sensor assembly after final trimming Please click here to view a larger version of this figure.
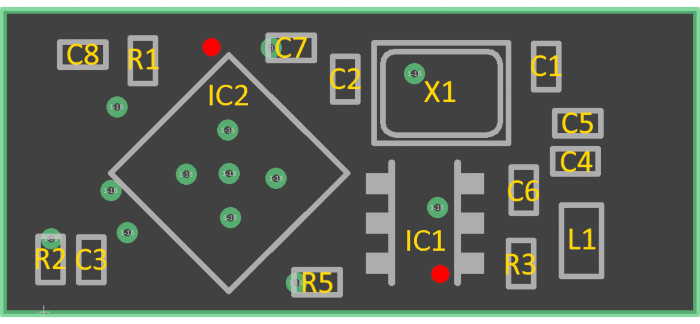
Figure 3: Placement diagram for the implantable sensor (see Table of Materials for component values). Pin 1 is marked as a red dot. Please click here to view a larger version of this figure.
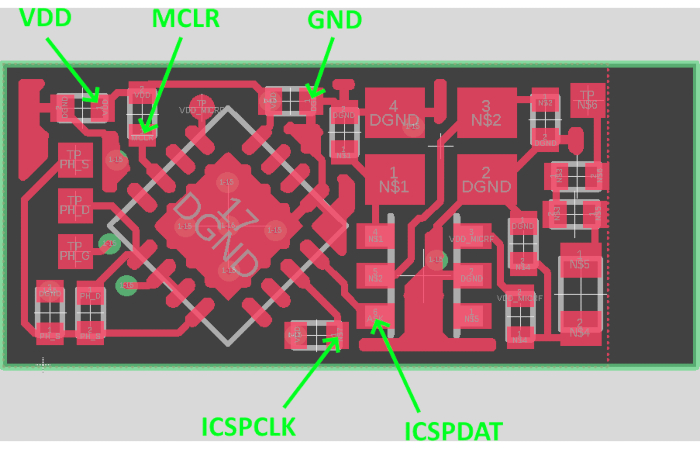
Figure 4: Placement of programming wires Please click here to view a larger version of this figure.
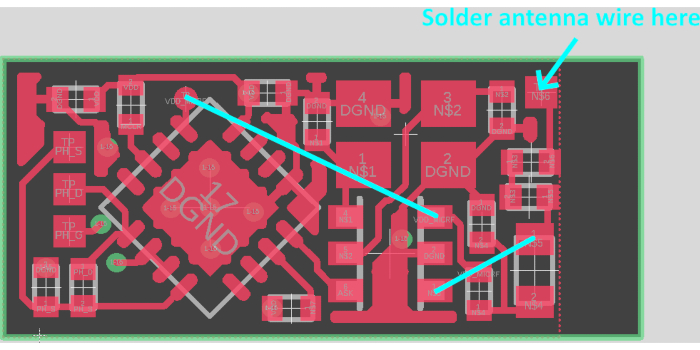
Figure 5: Placement of antenna wire and jumper wires Please click here to view a larger version of this figure.
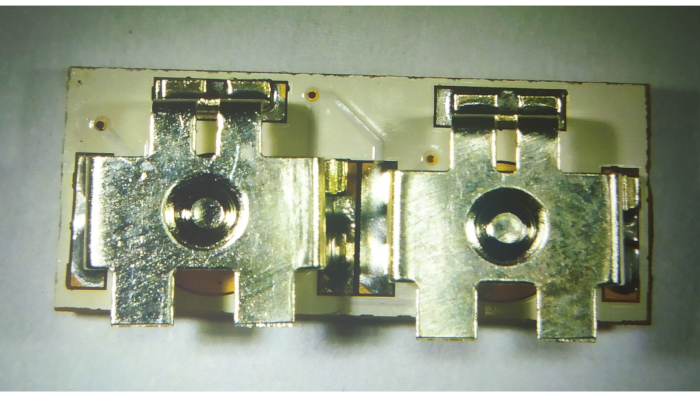
Figure 6: Placement of battery holders Please click here to view a larger version of this figure.
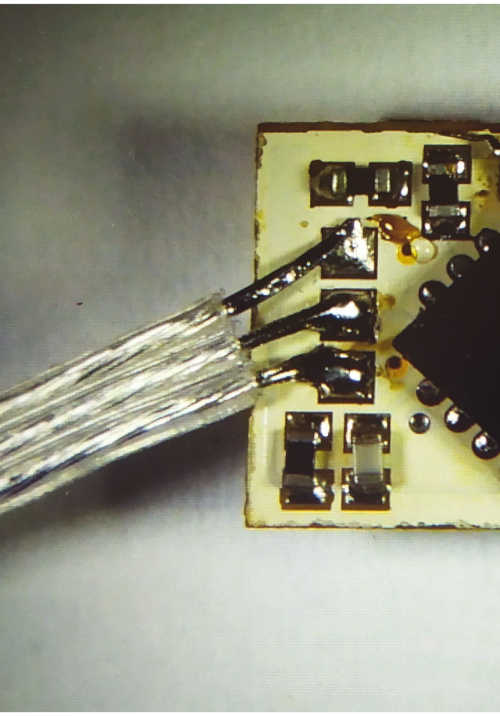
Figure 7: Soldering of the pH sensor assembly to the electronics Please click here to view a larger version of this figure.

Figure 8: Finished encapsulated sensor. (A) side view, (B) back view Please click here to view a larger version of this figure.
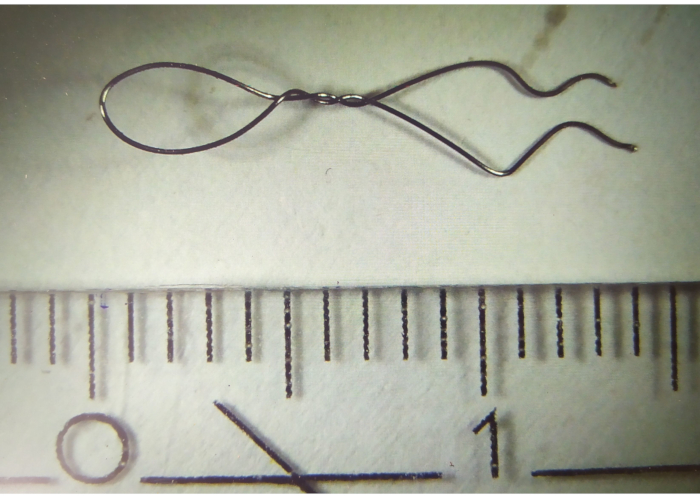
Figure 9: Titanium wire hook Please click here to view a larger version of this figure.

Figure 10: Attachment of the wire hook to the implantable device Please click here to view a larger version of this figure.
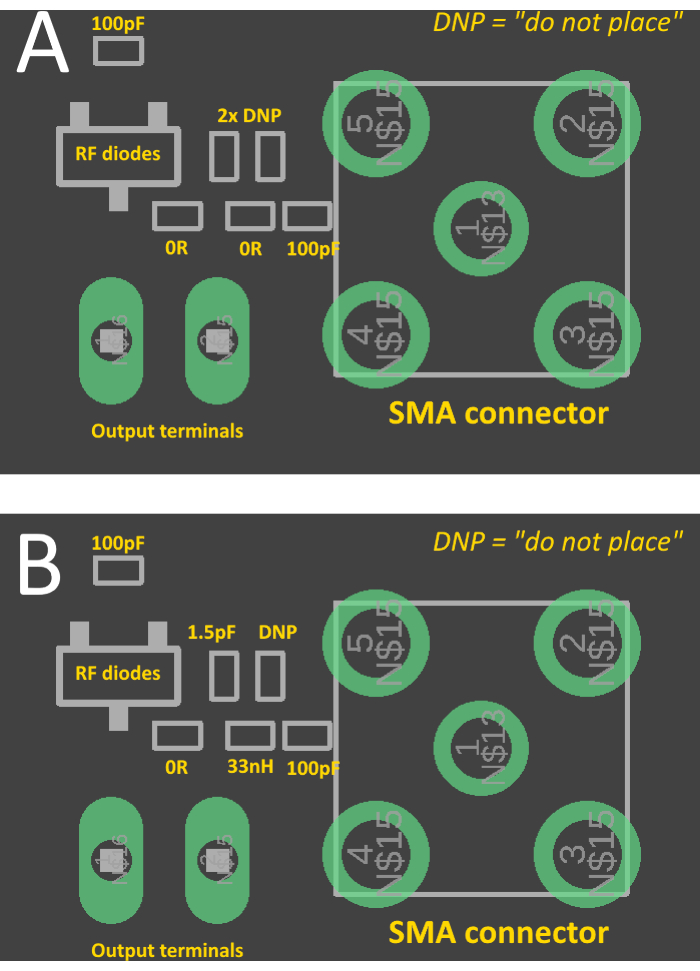
Figure 11: Placement diagram for the rectenna. (A) with matching components, (B) without matching components, ready to be matched with a vector network analyzer Please click here to view a larger version of this figure.
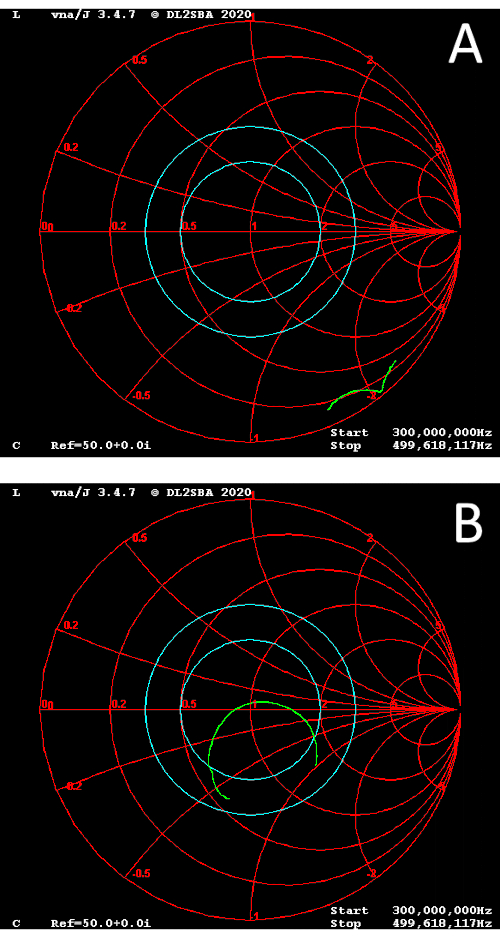
Figure 12: Smith chart. (A) unmatched rectenna, (B) matched rectenna Please click here to view a larger version of this figure.
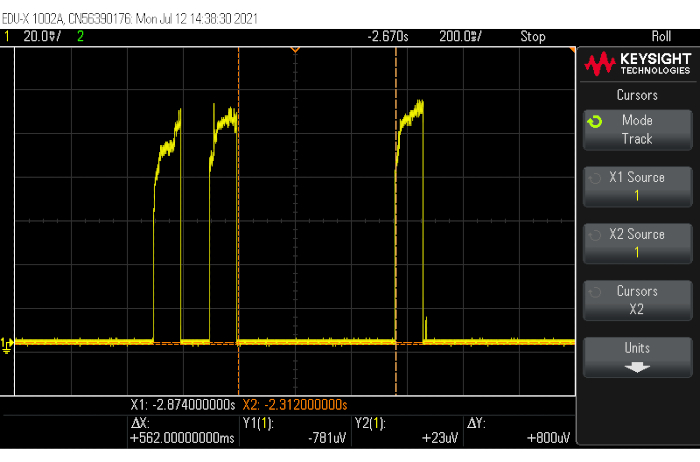
Figure 13: Example response of the rectenna to the incoming data from the sensor Please click here to view a larger version of this figure.
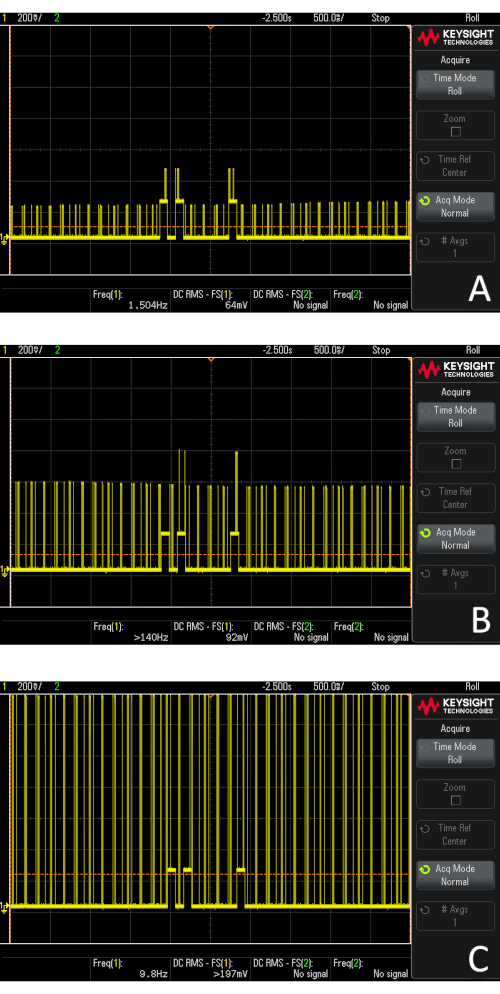
Figure 14: Example response when in the presence of RF noise (nearby phone with an active GSM call). (A) 20 cm between the edge of the phone and receiver, (B) 10 cm between the edge of the phone and receiver, (C) 5 cm between the edge of the phone and receiver Please click here to view a larger version of this figure.
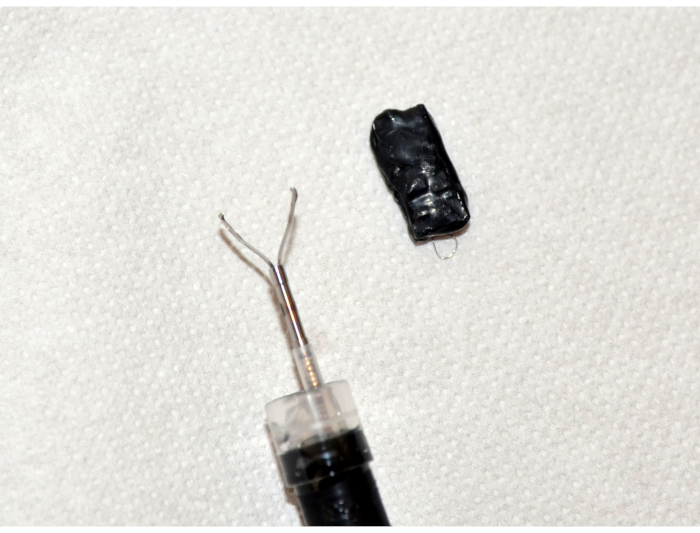
Figure 15: Picture of the endoscope with hemostatic clip and implantable pH sensor Please click here to view a larger version of this figure.
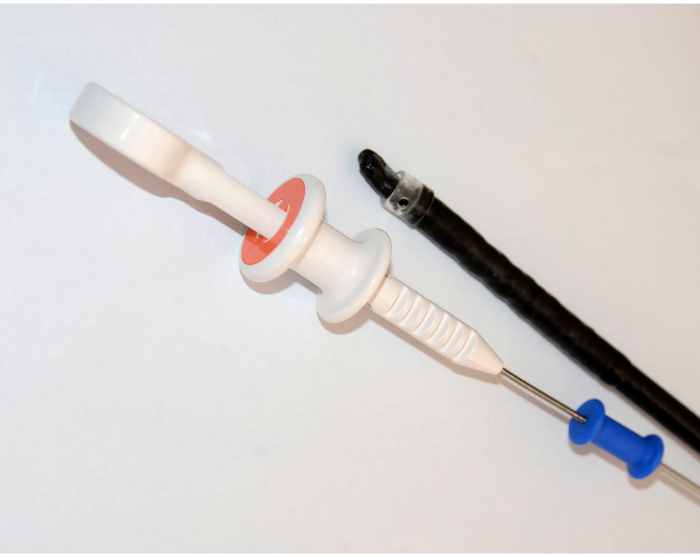
Figure 16: Implantable pH sensor grasped with the hemostatic clip in a cap Please click here to view a larger version of this figure.
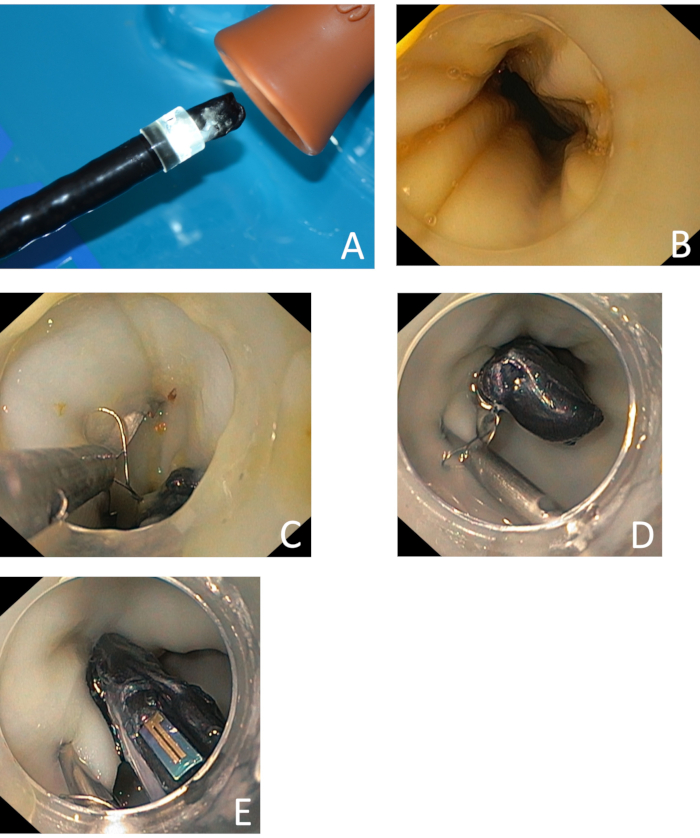
Figure 17: Implantation of the sensor. (A) insertion of the endoscope with the implantable pH sensor into the model, (B) place of implantation – 3 cm above the gastroesophageal junction, (C) preparation of the clip placement, (D) the clip was successfully placed, (E) view of the ISFET pH sensor, implanted to the proximity of lower esophageal sphincter Please click here to view a larger version of this figure.

Figure 18: Injection of the pH buffer solution through the endoscope channel Please click here to view a larger version of this figure.
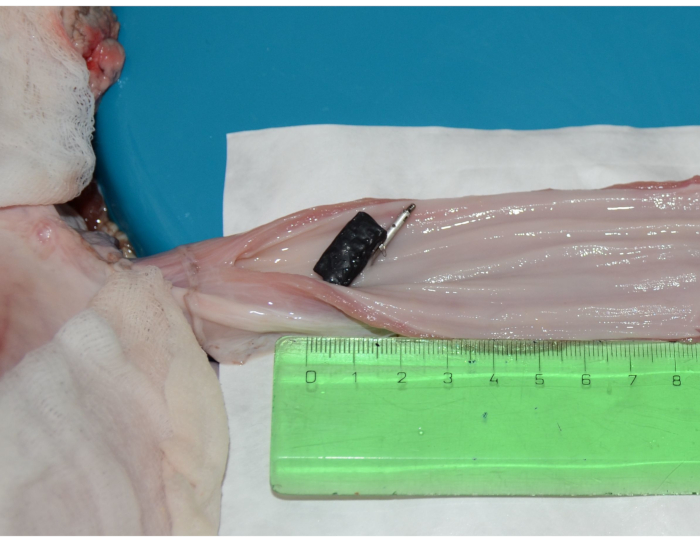
Figure 19: Dissected esophagus of the ex vivo model with the implanted sensor Please click here to view a larger version of this figure.
| Calibration data | ||
| pH value (cal. meter) [-] | Pulse length [ms] | Calc. volt. output [mV] |
| 3.98 | 400 | 1200 |
| 10.01 | 710 | 1510 |
Table 1: Example calibration data
| Measured data | ||||
| pH value (cal. meter) [-] | Calc. volt. output [mV] | Estimated pH [-] | Error [abs. pH] | Error [%] |
| 0.62 | 1010 | 0.28 | -0.34 | -54% |
| 3.98 | 1200 | 3.98 | 0.00 | 0% |
| 10.01 | 1490 | 9.62 | -0.39 | -4% |
| 0.62 | 1020 | 0.48 | -0.14 | -23% |
| 7.01 | 1350 | 6.90 | -0.11 | -2% |
| 3.98 | 1220 | 4.37 | 0.39 | 10% |
| 10.01 | 1480 | 9.43 | -0.58 | -6% |
| 3.98 | 1210 | 4.17 | 0.19 | 5% |
| 7.01 | 1350 | 6.90 | -0.11 | -2% |
| Std. deviation of pH [-] | 0.30 | |||
| Mean error [-] | 0.25 | |||
Table 2: Measured data (test with beakers)
| Measured data | ||||
| pH value (cal. meter) [-] | Calc. volt. output [mV] | Estimated pH [-] | Error [abs. pH] | Error [%] |
| 0.62 | 1010 | 0.28 | -0.34 | -54% |
| 3.98 | 1220 | 4.37 | 0.39 | 10% |
| 7.01 | 1340 | 6.70 | -0.31 | -4% |
| 10.01 | 1520 | 10.20 | 0.19 | 2% |
| Std. deviation of pH [-] | 0.36 | |||
| Mean error [-] | 0.31 | |||
Table 3: Measured data (test in an ex vivo model)
Supplemental File 1: spreadsheet.xlsx. Spreadsheet for calibrating and processing of the data from the sensor Please click here to download this File.
Supplemental File 2: pcb1.zip. Gerber manufacturing data for the implantable device Please click here to download this File.
Supplemental File 3: pcb2.zip. Gerber manufacturing data for the receiver Please click here to download this File.
Supplemental File 4: firmware_10s.zip. Firmware for the microcontroller with 10 s transmission period Please click here to download this File.
Supplemental File 5: firmware_1min.zip. Firmware for the microcontroller with 1 min transmission period Please click here to download this File.
Supplemental File 6: firmware-test.zip. Firmware for the microcontroller without 24 h pause before activation Please click here to download this File.
Supplemental File 7: Schematic diagram of the electronics Please click here to download this File.
