A prospective randomized study compared complete aspiration of synovial fluid from the knee and intra-articular injection with corticosteroid alone. It demonstrated that aspirating as much synovial fluid as possible can reduce the risk for recurrence of arthritic symptoms when treating rheumatoid arthritis patients with intra-articular corticosteroids. Figure 1 shows the reduction in the proportion of relapses in the arthrocentesis group3.
A retrospective chart review of arthrocenteses and joint injections compared the incidence of clinically significant bleeding in patients receiving warfarin with an international normalized ratio ≥2.0 and those whose anticoagulation was adjusted to an international normalized ratio <2.0. Table 1 shows no statistically significant difference in bleeding between the two groups6.
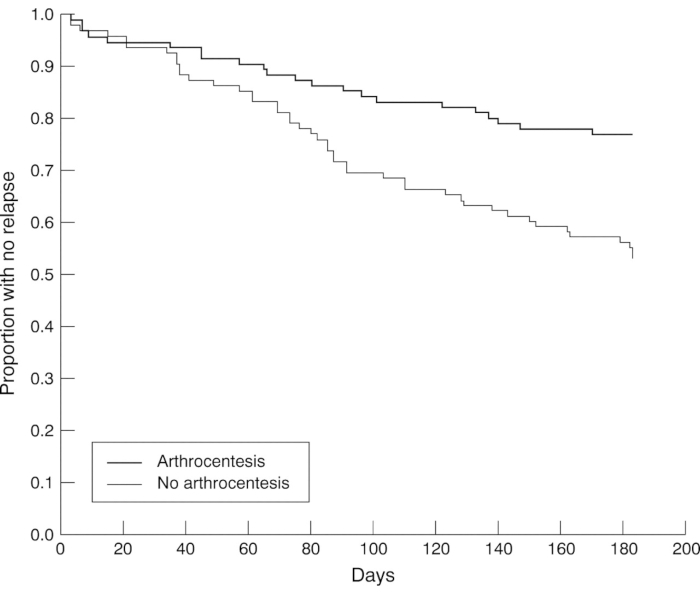
Figure 1: Proportion of arthritis relapse with or without arthrocentesis. The proportion of relapses in the arthrocentesis group was significantly reduced (p = 0.0009) and at the end of 6 months, there were 23% relapses in the arthrocentesis group and 47% in the no arthrocentesis group (p=0.001). Ninety-five knees were randomized to arthrocentesis and 96 had no arthrocentesis before triamcinolone hexacetanoide (20 mg) was injected into the inflamed knee joint. This figure is adapted with permission from Weitoft et al.3. Please click here to view a larger version of this figure.
| Complications | Group A (INR ≥ 2) (n = 456) | Group B (INR < 2) (n = 184) | P Value |
| Clinically significant bleeding (early) | 1 (0.2%) | 0 | NS |
| Clinically significant bleeding (late) | 0 | 0 | NS |
| Infection of joint (late) | 1 (0.2%) | 0 | NS |
| Pain of joint causing physician visit | 3 (0.7%) | 0 | NS |
| INR=international normalized ratio; NS=not significant. | |||
Table 1: Early and late complications between two groups. Procedure-related complications were defined as early (within 24 h) and late (within 30 days) clinically significant bleeding in or around a joint, infection of joint related to the arthrocentesis, and pain requiring a physician visit excluding chronic pain. Four patients accounted for 5 complications. This table has been modified with permission from Ahmed et al.6.
