Representative results from three bullous keratopathy patients with extensive anterior synechia who had a well-controlled IOP after lens extraction, anterior vitrectomy, and IOL implantation to cure malignant glaucoma are described in the study. In these cases, one received conventional anterior chamber plasty with synechia separation and penetrating keratoplasty (PKP), the other two received PSACP first, and then received Descemet's stripping automated endothelial keratoplasty (DSAEK) or PKP. Postop reaction and pigment release of all three cases were mild and faded within 4 weeks under routine anti-infection and anti-inflammatory eye drops. The prognosis of these three patients was compared on different days after 360° PAS appearance with the ASOCT (1-day post-operation) or UBM (12 weeks or 24 weeks post-operation) after the anterior chamber plasty surgery.
Case 1
A 68-year-old female was diagnosed with bullous keratopathy and extensive anterior synechia in her right eye from IOP-well-controlled (21 mmHg with four kinds of anti-glaucoma eye drops) malignant glaucoma. She already had lens extraction, anterior vitrectomy, and IOL implantation. Her right eye's best-corrected visual acuity (BCVA) was 20/4000. The iris's extensive anterior synechia was shown with ASOCT and UBM (Figure 1 and Figure 2).
She received anterior chamber plasty with synechia separation and penetrating keratoplasty (PKP) in her right eye. One-day post-surgery (Figure 4), she showed no PAS with the ASOCT (Figure 4C), and BCVA improved to 20/1000 with elevated IOP (32 mmHg). However, 12 weeks after surgery, she showed 360° PAS with the UBM (Figure 4D), and BCVA decreased to 20/1600. At that moment, IOP was uncontrolled over 25 mmHg, and the bullous keratopathy reoccurred.
Case 2
A 75-year-old female was diagnosed with bullous keratopathy and extensive anterior synechia in her left eye from IOP-well-controlled (18 mmHg with three kinds of anti-glaucoma eye drops) malignant glaucoma, which already had lens extraction, anterior vitrectomy, and IOL implantation. BCVA of her left eye was 20/1600. The disappearance of the anterior chamber was observed with ASOCT and UBM (Figure 5).
She received PSACP, where pentagram sutures were placed as a barrier in front of the anterior surface of the iris (Figure 6). No PAS was seen with ASOCT or UBM from day 1 till 12 weeks post-surgery (Figure 7). Then, she received DSAEK. On 24 weeks post-PSACP, no corneal edema was observed with ASOCT, and one clock hour PAS was demonstrated with UBM (Figure 8), with BCVA 20/66. IOP remained normal without any medication post-surgery.
Case 3
A 69-year-old female was diagnosed with bullous keratopathy and extensive anterior synechia in her right eye from IOP-well-controlled (12 mmHg with four kinds of anti-glaucoma eye drops) malignant glaucoma, which was post lens extraction, anterior vitrectomy, IOL implantation, and DSAEK. The BCVA of her right eye was 20/1600. Extensive PAS was shown with ASOCT and UBM (Figure 9).
She received PSACP and showed 2 clock hours PAS with ASOCT on day 1 post-surgery, and she missed the 12-week-follow-up. As she showed 6 clock hours PAS with UBM in 24 weeks post-surgery (Figure 10), she received PKP. During PKP, the suture was broken accidentally and then removed. On 1-week post PKP, she showed mild edema in the cornea graft and 6 clock hours PAS with the ASOCT (Figure 11) with improved BCVA 20/400. IOP remained normal without any medication post-surgery. Unfortunately, she did not follow up.
Comparisons
BCVA, IOP, cornea or corneal graft, anterior synechia of iris were found in these three patients preoperationally and post-operationally (Table 1 and Table 2). The prognosis of Case 2 and Case 3 was significantly better than in Case 1.
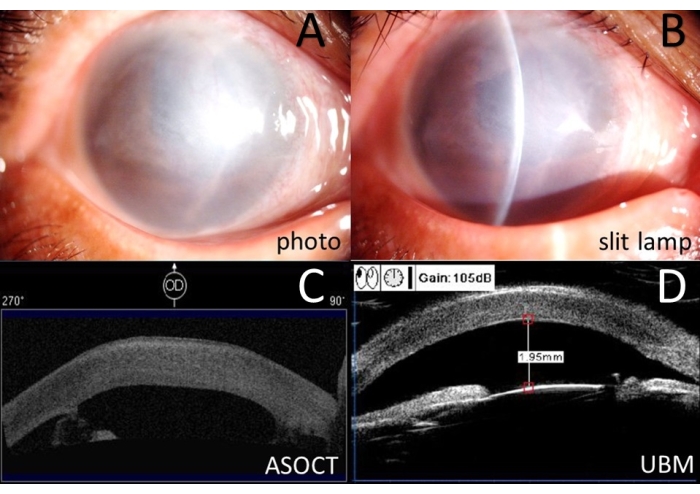
Figure 1: Preoperative examinations for Case 1. (A) Anterior segment photography. (B) Color slit-lamp photography. (C) Anterior segment optical coherence tomography (ASOCT). (D) Ultrasound biomicroscopy (UBM). Please click here to view a larger version of this figure.
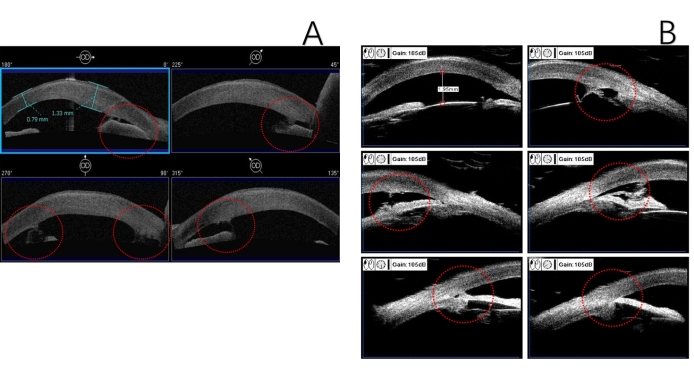
Figure 2: Assessment of anterior synechia of iris for Case 1. (A) Anterior segment optical coherence tomography. (B) Ultrasound biomicroscopy. Red circle: anterior synechia of the iris. Please click here to view a larger version of this figure.
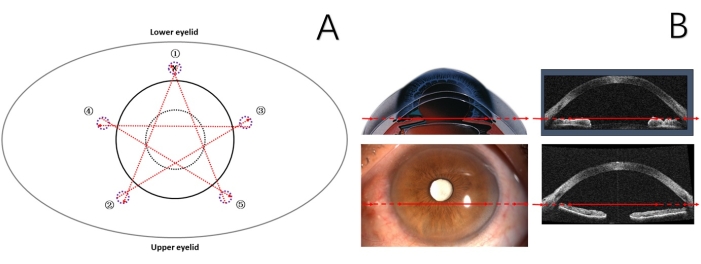
Figure 3: Schematic representation of the procedure of PSACP for Case 3. (A) Black dashed circle: pupil; black circle: limbus; purple dashed circle: the mark of scleral puncture point; numbers and red arrow: suturing sequence and direction, both ends of the red arrow represent the exact puncture points; X: the surgical knot. (B) Red arrow: suturing position and direction. PSACP = Pentagram Suturing Anterior Chamber Plasty. Please click here to view a larger version of this figure.
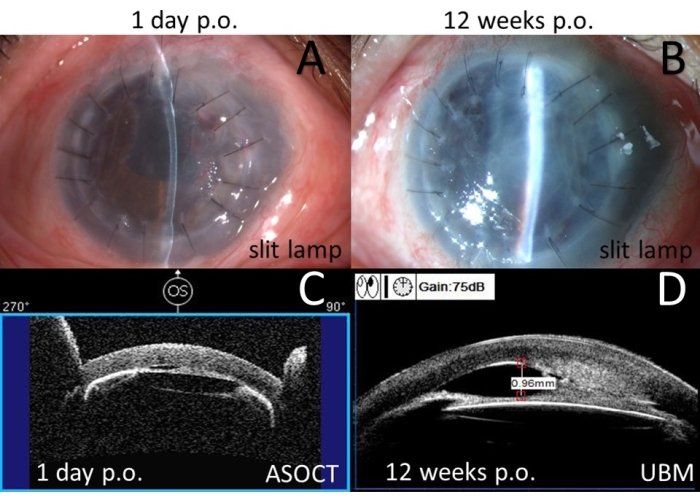
Figure 4: Postoperative examinations for Case 1. (A) Color slit lamp photography on day 1 post-operation. (B) Color slit lamp photography in 12 weeks post-operation. (C) Anterior segment optical coherence tomography (ASOCT) on day 1 post-operation. (D) Ultrasound biomicroscopy (UBM) in 12 weeks post-operation. Please click here to view a larger version of this figure.
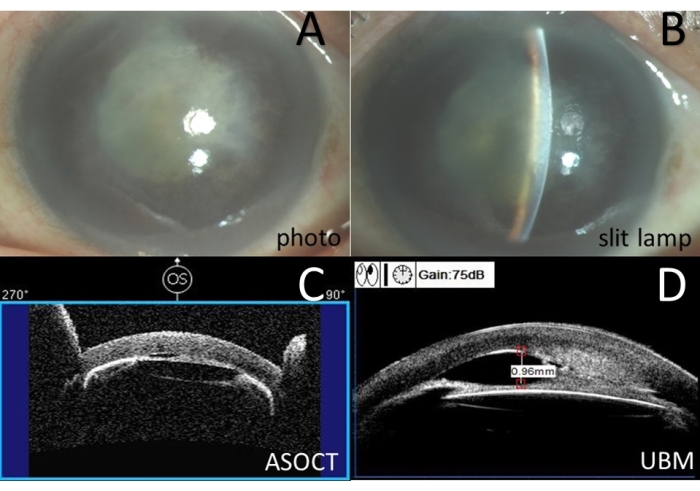
Figure 5: Preoperative examinations for Case 2. (A) Anterior segment photography. (B) Color slit-lamp photography. (C) Anterior segment optical coherence tomography (ASOCT). (D) Ultrasound biomicroscopy (UBM). Please click here to view a larger version of this figure.
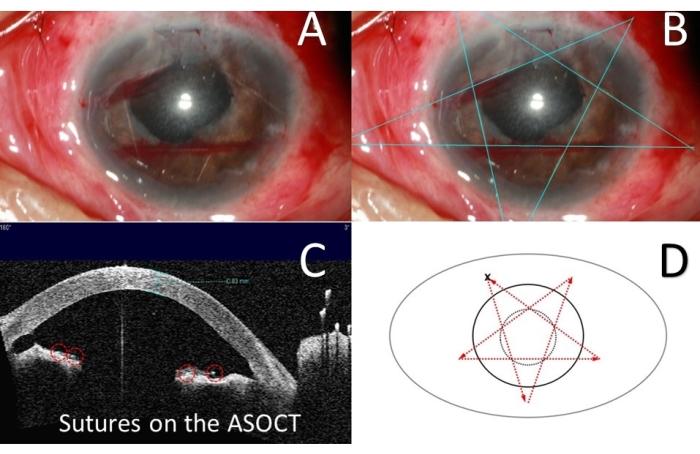
Figure 6: Diagrammatic sketches of PSACP in operation for Case 2. (A) Color photography for sutures. (B) Blueline: pentagram sutures. (C) Anterior segment optical coherence tomography (ASOCT) on day 1 post-operation, red circle: sutures. (D) Black dashed circle: pupil; black circle: limbus; red arrow: suturing direction; X: the surgical knot. PSACP = Pentagram Suturing Anterior Chamber Plasty. Please click here to view a larger version of this figure.
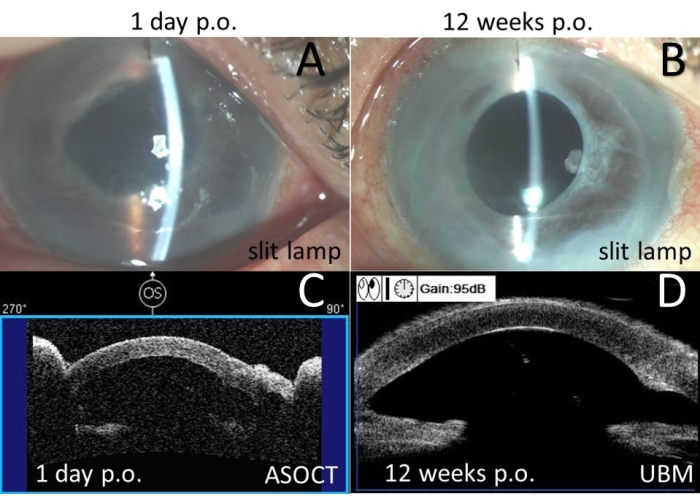
Figure 7: Postoperative examinations for Case 2. (A) Color slit lamp photography on day 1 post-operation. (B) Color slit lamp photography in 12 weeks post-operation. (C) Anterior segment optical coherence tomography (ASOCT) on day 1 post-operation. (D) Ultrasound biomicroscopy (UBM) in 12 weeks post-operation. Please click here to view a larger version of this figure.
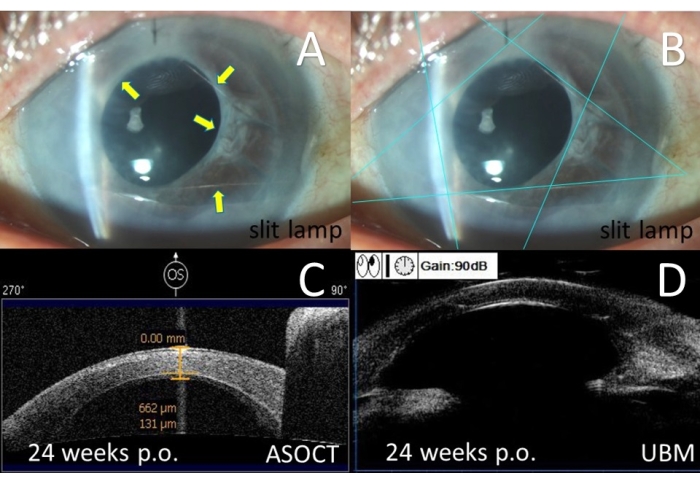
Figure 8: Postoperative examinations for Case 2 in 24 weeks post PSACP. (A) Color slit lamp photography, yellow arrow: sutures in the anterior chamber. (B) Color slit lamp photography, blue line: pentagram sutures. (C) Anterior segment optical coherence tomography (ASOCT) showed the cornea and endothelium graft. (D) Ultrasound biomicroscopy (UBM). PSACP = Pentagram Suturing Anterior Chamber Plasty. Please click here to view a larger version of this figure.
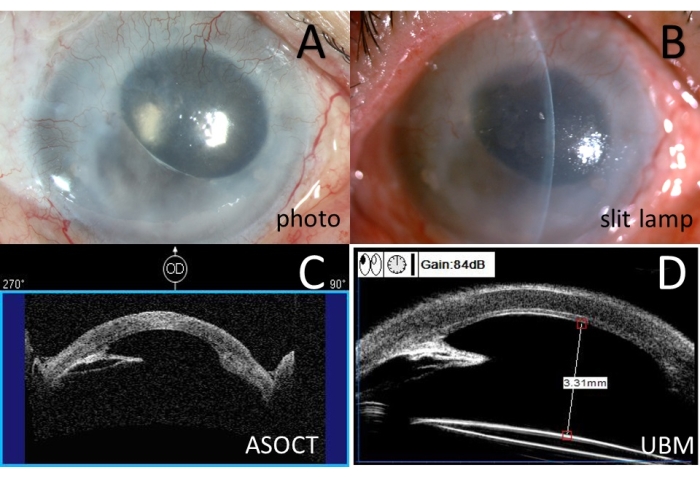
Figure 9: Preoperative examinations for Case 3. (A) Anterior segment photography. (B) Color slit-lamp photography. (C) Anterior segment optical coherence tomography (ASOCT). (D) Ultrasound biomicroscopy (UBM). Please click here to view a larger version of this figure.
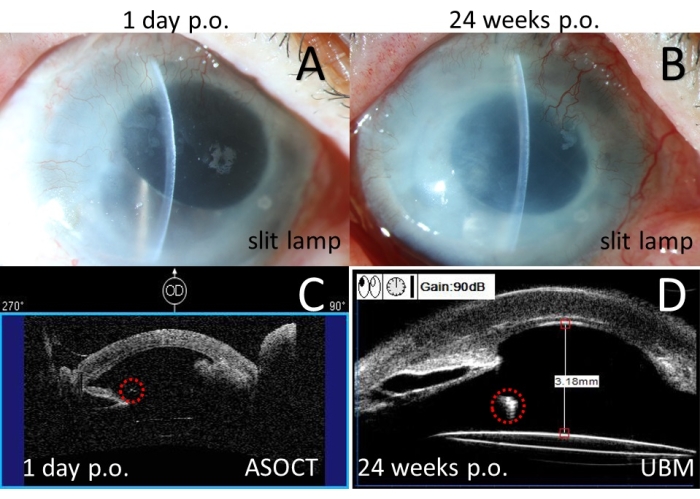
Figure 10: Postoperative examinations for Case 3. (A) Color slit lamp photography on day 1 post-operation. (B) Color slit lamp photography in 24 weeks post-operation. (C) Anterior segment optical coherence tomography (ASOCT) on day 1 post-operation. (D) Ultrasound biomicroscopy (UBM) in 24 weeks post-operation. Red circle: sutures. Please click here to view a larger version of this figure.
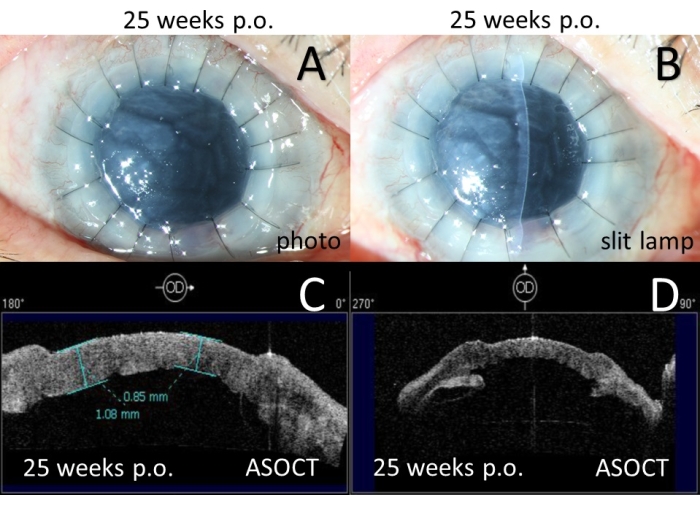
Figure 11: Postoperative examinations for Case 3 in 25 weeks post PSACP. (A) Anterior segment photography in 1 week post PKP. (B) Color slit lamp photography in 1 week post PKP. (C) Anterior segment optical coherence tomography (ASOCT) showed the cornea and graft. (D) Anterior segment optical coherence tomography (ASOCT) showed anterior synechia of the iris. PSACP = Pentagram Suturing Anterior Chamber Plasty. PKP = penetrating keratoplasty. Please click here to view a larger version of this figure.
| Case | Kind of surgery | BCVA | IOP (mmHg) | Kind of anti-glaucoma eye drops | |||
| Pre-op. | Postop. | Pre-op. | Postop.* | Pre-op. | Postop. | ||
| 1 | CACP+PKP | 20/4000 | 20/1600 | 21 | 25 | 4 | 3 |
| 2 | PSACP, DSAEK | 20/1600 | 20/66 | 18 | 13 | 3 | 0 |
| 3 | PSACP, PKP | 20/1600 | 20/400 | 12 | 14 | 3 | 0 |
Table 1: Visual acuity, intraocular pressure, and medications of the presented cases. BCVA = best-corrected visual acuity; IOP = intraocular pressure; Pre-op. = pre-operational; Postop. = post-operational; CACP = conventional anterior chamber plasty; PKP = penetrating keratoplasty; PSACP = Pentagram Suturing Anterior Chamber Plasty; DSAEK = Descemet's stripping automated endothelial keratoplasty.
| Case | Kind of surgery | Cornea/Corneal graft edema | Anterior synechia of iris (ASOCT) | Anterior synechia of iris (UBM) | |||
| Pre-op. | Postop. | Pre-op. | Postop.* | Pre-op. | Postop. | ||
| 1 | CACP+PKP | Yes | No | 8CH | No | 9CH | 9CH |
| 2 | PSACP, DSAEK | Yes | No | 12CH | No | 12CH | 1CH |
| 3 | PSACP, PKP | Yes | No | 12CH | 2CH | 12CH | 6CH# |
Table 2: Clinical characteristics of cornea and iris of the presented cases. ASOCT = anterior segment optical coherence tomography; UBM = Ultrasound biomicroscopy; Pre-op. = preoperational; Postop. = post operational; CACP = conventional anterior chamber plasty; PKP = penetrating keratoplasty; CH = clock hour; PSACP = Pentagram Suturing Anterior Chamber Plasty; DSAEK = Descemet's stripping automated endothelial keratoplasty. * = 1 day post PSACP. # = 24 weeks post PSACP.
