Anesthesia of 10-day-old mice. The10-day-old pups can be anesthetized with 4.5% isoflurane in 4-5 min; however, they recover from anesthesia in the process of preparation for intubation. Due to their small size, intubation under isoflurane anesthesia delivered by a standard nose cone is not feasible. We have previously used a ketamine/xylazine/atropine anesthetic regimen of 100/13/0.5 mg/kg, respectively, for cardiothoracic surgery in 15- and 21-day-old pups and adults4,7. In preliminary experiments, that included oxygen supplementation, it was found that the recommended injectable regimen of 50-150 mg/kg ketamine and 5-10 mg/kg xylazine10 resulted in an unacceptable mortality in 10-day-old pups. Given the inverse correlation between body weight and litter size of 10-day-old pups (R2 = 0.250, p < 0.0001; Figure 2), we titrated the anesthetic regimen according to body weight groupings. Reducing the ketamine/xylazine/atropine dosage to 50/6/0.18 mg/kg, respectively, resulted in a sufficient depth of anesthesia to allow endotracheal intubation of spontaneously breathing pups weighing 5.5-8.10 g (Table 1), but this dose was not tolerated by lighter pups. Reducing the ketamine/xylazine/atropine dosage to 30/4/0.12 mg/kg, respectively, enabled intubation of pups weighing 4.50-5.49 g, while further reduction of the ketamine dosage to 20 mg/kg enabled intubation of pups weighing 3.15-4.49 g (Table 1). Table 1 shows the number and percentage of intubated pups that proceeded to surgery; however, it is difficult to extract from this data anesthesia-related mortality from mortality associated with too many intubation attempts. In the interest of reducing animal wastage, we did not specifically quantitate anesthesia-related mortality.
Intubation of 10-day-old mice. Outcomes were best when intubation was achieved after only one or two attempts. Pups with a lower body weight were more difficult to intubate than heavier pups and required more attempts (p < 0.001; Table 1). Survival post-intubation correlated with body weight with 59%, 70%, and 80% survival for low-, mid-, and high-weight groups, respectively (R2 = 0.995, p = 0.04; Table 1).
Myocardial infarction surgery of 10-day-old mice. Pups were monitored for 2 days after surgery. There were no signs of pain post-surgery. Of the pups that did not survive to follow-up at 48 h (Table 1), one from the low-weight group died 6 h after surgery, one pup from each of the mid- and high-weight groups died before being placed back with the dam, and one pup from each of the mid- and high-weight groups were cannibalized by the dam within 16 h of surgery, with small body parts or nothing remaining the next morning. Survival 2 days after myocardial infarction surgery was consistent between the different weight groups at 86%-92% (p = 0.91; Table 1). Infarcted myocardium, as assessed 2 days post-surgery by Alcian-blue perfusion of the heart, was evident by clear demarcation of stained, non-infarcted (blue) from ischemic (unstained) tissue, distal to the ligation (Figure 1E).
Overall survival for the entire procedure (intubation plus surgery) correlated with pup body weight at 55%, 60%, and 70% for low-, mid-, and high-weight groups, respectively (R2 = 0.978, Table 1), although this correlation did not achieve statistical significance (p = 0.09).
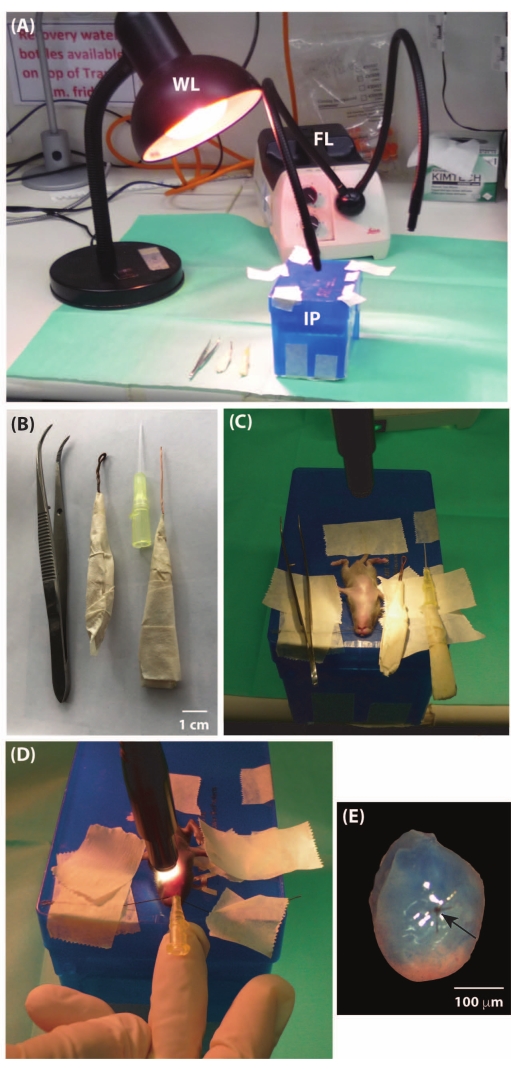
Figure 1: Endotracheal intubation of a 10-day-old C57BL/6J mouse pup. (A) Intubation set-up showing large warming lamp (WL), intubation platform (IP), and flexible fiber-optic lighting (FL) used to aid visualization of the vocal cords at the time of intubation. (B) Forceps, laryngoscope, 24-gauge cannula that is used as an endotracheal tube, and a piece of copper wire that is inserted into the endotracheal tube via the luer lock adaptor to stiffen the cannula during intubation (scale bar = 1 cm). (C) The anesthetized pup is secured supine by taping the tail and front limbs onto the intubation platform (12 cm (L) x 8.5 cm (W) x 7.5 cm (H)). A thread placed over the incisors is used to extend the head and is taped in position. (D) The fiber-optic light is placed over the neck to trans-illuminate the trachea just below the vocal cords. The tongue is held with small forceps, and then movement of the vocal cords is visualized by exposing the glottis with the laryngoscope. The endotracheal tube is inserted into the trachea while the vocal cords are open. (E) Photograph of a representative mouse pup heart perfused with Alcian blue (frontal view with the base of the heart at the top and apex at the bottom, and atria removed) 48 h post-ligation (black suture, black arrow) of the left coronary artery taken under a surgical microscope (10x objective) mounted with a camera. Non-infarcted myocardium is stained blue, infarcted myocardium at the apex is unstained and pale; scale bar = 100 µm. This figure has been modified from17. Please click here to view a larger version of this figure.
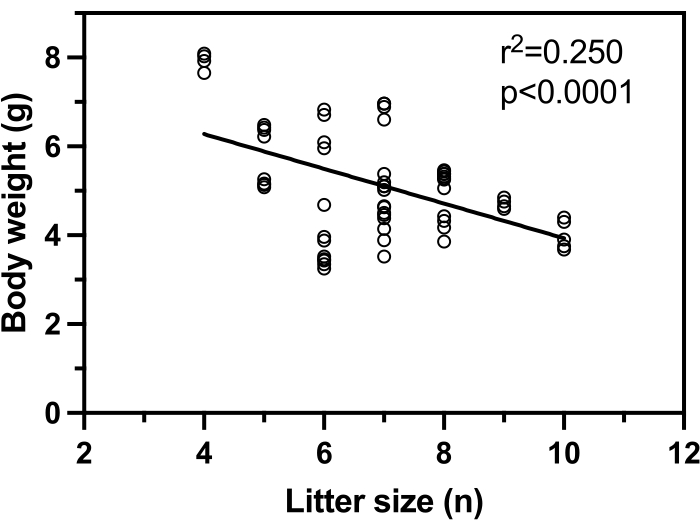
Figure 2: Body weight of 10-day-old C57BL/6 pups is inversely correlated with litter size. Pups were from litters ranging in size from 4-10. The average C57BL/6 litter size is seven18. Data were analyzed by simple linear regression, with p < 0.05 being considered significant. This figure has been modified from17. Please click here to view a larger version of this figure.
| Anesthesia regimen: ketamine/ xylazine/ atropine (mg/kg); given in 10 mL/g body weight, ip | Body weight, g | Number of pups studied | Intubation attempts (A, 1-2; B, 3-4 or C, >4) and number of pups intubated, n (%) | Intubated pups proceeding to surgery, n (%) | Survival two days post-surgery, n (%) | Overall survival after intubation plus surgery, n (%) | ||
| A | B | C | ||||||
| 20/4/0.12 | 3.15 – 4.49 | 22 | 8 (36) | 9 (41) | 5 (23) | 13 (59) | 12 (92) | 12 (55) |
| 30/4/0.12 | 4.50 – 5.49 | 20 | 13 (65) | 5 (25) | 2 (10) | 14 (70) | 12 (86) | 12 (60) |
| 50/6/0.18 | 5.50 – 7.30 | 20 | 13 (65) | 3 (15) | 4 (20) | 16 (80) | 14 (88) | 14 (70) |
| p (Chi-square test) | p<0.001 | p=0.91 | ||||||
| R2 (Correlation coefficient, | 0.995, | 0.978, | ||||||
| p value) | p=0.04 | p=0.09 | ||||||
Table 1: Anesthesia regimen, number of intubation attempts, and post-procedure survival of 10-day-old mouse pups. Data were analyzed by Chi-squared test, with p < 0.05 being considered significant.
