Regarding the normal model, good LV contraction was successfully established after de-clamping. The ischemia time of the transplanted heart and the recipient's anesthesia time were approximately 60 min and 130 min, respectively (Table 1).
Good LV contraction was also obtained after de-clamping in the new AR model. The ischemic time of the transplanted heart and the recipient's anesthesia time in the AR model were approximately 5 min and 10 min longer than the times of the normal model (Table 2). The AR model showed significantly larger LV dimensions and a thinner LV wall than the normal model (Table 3), and postoperative echocardiography detected an AR jet flow in the AR model (Figure 3). Macroscopic examination showed LV dilation and endocardial thickening (Figure 4), and the Masson's Trichrome-stained samples demonstrated fibrotic changes in the myocardium and endocardium (Figure 5). In contrast, these fibrotic changes were not found in the normal model.
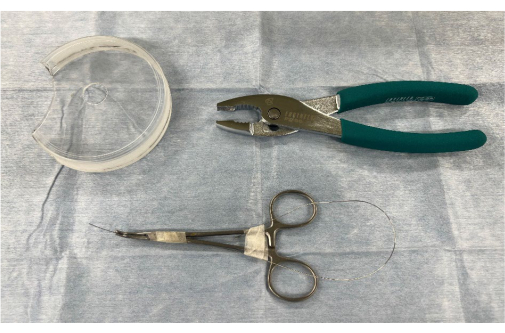
Figure 1: Surgical instruments and materials for creating an aortic regurgitation model using heterotopic abdominal heart transplantation. 1, a modified Petri dish with a hole in the center; 2, pliers; and 3, a stiff guidewire Please click here to view a larger version of this figure.
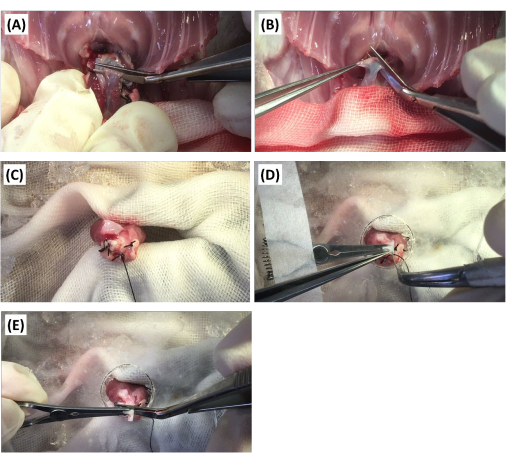
Figure 2: Surgical procedure for the creation of the aortic regurgitation model. (A) The donor's pulmonary artery is transected using Potts scissors. (B) The donor's ascending aorta is transected distally to the brachiocephalic artery with Potts scissors. (C) The donor's heart is fixed with pliers. (D) After the donor's ascending aorta is fixed with a vascular clip, the aortic valve is punctured with a stiff guidewire. (E) The aorta is transected proximally to the brachiocephalic artery using Potts scissors. Please click here to view a larger version of this figure.
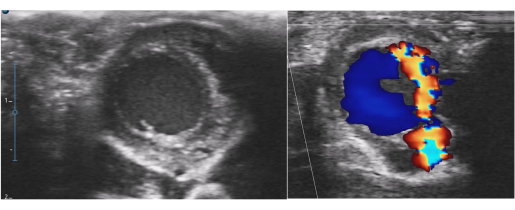
Figure 3: Postoperative echocardiography for the aortic regurgitation model. Left ventricular dilatation and a severe aortic regurgitation jet flow were detected. Please click here to view a larger version of this figure.

Figure 4: Macroscopic findings of the aortic regurgitation model. Left ventricular dilatation and endocardial thickening were confirmed. Please click here to view a larger version of this figure.
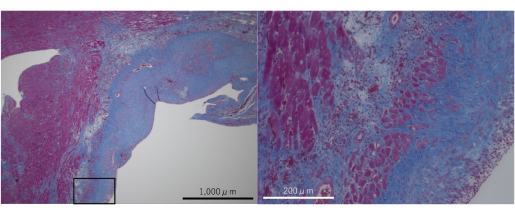
Figure 5: Masson's Trichrome-stained microphotographs of the aortic regurgitation model. Fibrotic changes were confirmed in the myocardium and endocardium. Please click here to view a larger version of this figure.
| Variables | Number | Variables | Number |
| Donor weight (g) | 236.0±40.6 | PA anastomosis time (min) | 18.8±2.7 |
| Recipient weight (g) | 294.6±43.6 | Ischemia time (min) | 59.7±4.8 |
| Clamp time (min) | 48.5±3.0 | ||
| Harvest time (min) | 16.5±2.0 | Anesthesia time (min) | 132.7±8.6 |
| Ao anastomosis time (min) | 26.9±2.7 | Extubation time (min) | 39.0±19.2 |
Table 1: Operative records of the normal model generated using heterotopic abdominal heart transplantation in rats (n = 19). Continuous variables are expressed as the mean ± standard deviation. Abbreviations: Ao = aorta; PA = pulmonary artery
| Variables | Number | Variables | Number |
| Donor’s weight (g) | 211.5±46.9 | PA anastomosis time (min) | 18.8±2.1 |
| Recipient’s weight (g) | 261.2±42.0 | Ischemia time (min) | 65.7±7.2 |
| Clamp time (min) | 49.3±4.9 | ||
| Harvest time (min) | 17.3±2.2 | Anesthesia time (min) | 143.7±14.6 |
| Ao anastomosis time (min) | 28.2±3.6 | Extubation time (min) | 28.0±14.5 |
Table 2: Operative records of the aortic regurgitation model generated using heterotopic abdominal heart transplantation in rats (n = 40). Continuous variables are expressed as the mean ± standard deviation. Abbreviations: Ao = aorta; PA = pulmonary artery
| Variables | Normal model | AR model | P value |
| LV wall (mm) | 3.05±0.50 | 2.19±0.57 | 0.002 |
| LVDd (mm) | 2.23±0.55 | 4.56±2.13 | 0.003 |
| LVDs (mm) | 1.32±0.34 | 3.30±1.79 | 0.003 |
| LV-FS (%) | 40.49±9.41 | 29.06±8.24 | 0.008 |
Table 3: Postoperative echocardiography data of the normal and AR models created using heterotopic abdominal heart transplantation in rats. Continuous variables are expressed as the mean ± standard deviation. A Student's t-test was used to compare the differences between the two groups (P < 0.05). Abbreviations: AR = aortic regurgitation; FS = fractional shortening; LV = left ventricular; LVDd = left ventricular end-diastolic diameter; LVDs = left ventricular end-systolic diameter.
