Incidence of pathological upgrade in gastric LGIN patients after ESD
A total of 120 gastric LGIN patients were included in this study, of which 49 (40.83%) experienced pathological upgrades after ESD. Among them, 42 cases were upgraded to HGIN, 1 case was upgraded to advanced gastric cancer, and 6 cases were upgraded to EGC. A total of 71 cases did not experience pathological upgrade, among which 2 cases were downgraded to inflammation, and 69 cases remained as LGIN, with a rate of pathological downgrade of 1.67%.
Univariate analysis of pathological upgrade after ESD in gastric LGIN patients
As shown in Table 1, there were no statistically significant differences (p > 0.05) in gender, HP infection, lesion location, surface nodules, presence of a demarcation line (DL) in the ME layer, lesion morphology, microstructure (MS), and microvascular (MV) morphology between the postoperative pathological upgrade group and the non-upgrade group of gastric LGIN patients. However, there were statistically significant differences (p < 0.05) in age, lesion size, gastric mucosal congestion, and surface ulceration and erosion.
Multivariate logistic regression analysis of pathological upgrade after ESD in gastric LGIN patients
Factors with p < 0.05 screened out by univariate analysis, including age, lesion size, gastric mucosal congestion, and surface ulceration and erosion, which were used as independent variables, and pathological upgrade after ESD in gastric LGIN patients was used as the dependent variable for logistic regression analysis (Table 2). Table 3 showed that age ≥60 years, lesion diameter ≥2 cm, gastric mucosal congestion, and surface ulceration and erosion were independent risk factors for pathological upgrade after ESD in patients with gastric LGIN. The final joint probability prediction model was P = 1 / [1 + e(26.515-0.161xβ1-0.357xβ2+0.039xβ3-0.269xβ4)] based on the prediction formula for logistic regression: P(y = 1/x) = 1/(1+e-(β0+β1×1+β2×2+β3×3+β4×4)), where y represents the dichotomous dependent variable, x represents the vector of independent variables, β represents the regression coefficient, and e represents the base of the natural logarithm. Additionally, technical term abbreviations will be defined when first used. This formula indicates that given the independent variable x, the probability of event y = 1 occurring is P(y = 1/x). When the sum of β0 + β1 x 1 + β2 x 2 + β3 x 3 + β4 x 4 increases, so too does the value of P(y = 1/x), indicating a higher probability of the event y = 1 occurring; and conversely, a lower probability of the event y = 1 occurring. Here, β1 is the regression coefficient of age, β2 is the regression coefficient of lesion size, β3 is the regression coefficient of gastric mucosal congestion, and β4 is the regression coefficient of surface ulceration and erosion.
Case presentation
As a representative case, a 50-year-old female patient presented with rough mucosa and erosion at the gastric angle during a physical examination. The endoscopic biopsy confirmed low-grade intraepithelial neoplasia (LGIN). Further investigations using magnification endoscopy, narrow band imaging (NBI), and pigment endoscopy suggested the patient was at risk of developing high-grade intraepithelial neoplasia (HGIN). The patient was advised to undergo endoscopic submucosal dissection (ESD) treatment, and the final pathological diagnosis was HGIN (as indicated in Figure 1).
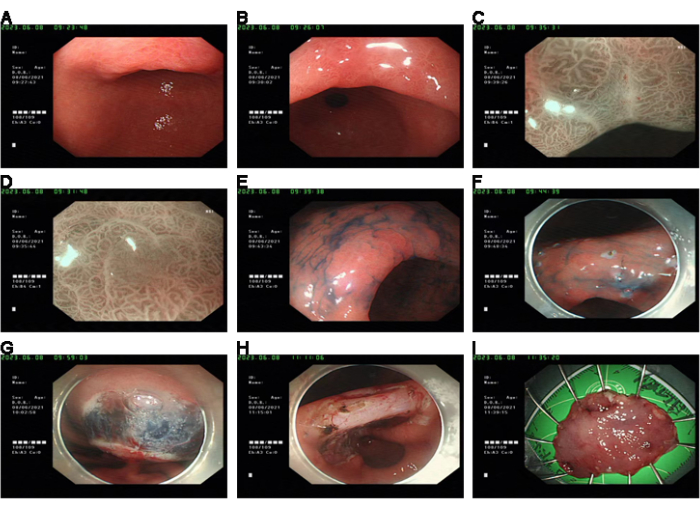
Figure 1: Case presentation. (A,B) Pre-operation, WLE showed rough gastric mucosa with erosion. (C,D) Irregular MV and MS were observed in the lesions observed by ME + NBI. (E) The contours of the lesions could be seen by indigo blush staining. (F) The lesions were labeled under the endoscope. (G) Stripped after submucosal water injection. (H) Wound hemostatic treatment. (I) Fixed specimens were sent for pathological examination. Please click here to view a larger version of this figure.
Table 1: Univariate analysis of post-ESD pathological upgrade (%). Please click here to download this Table.
Table 2: Multivariate logistic regression analysis variable assignment table for post-ESD pathological upgrade. Please click here to download this Table.
Table 3: Multivariate logistic regression analysis of post-ESD pathological upgrade. Please click here to download this Table.
