The following protocol follows the University of Michigan (UMICH) Institutional Animal Care and Use Committee (IACUC) policies and guidelines, the U.S. Government Principles for the Utilization and Care of Vertebrate Animals Used in Testing, Research, and Training, and the ARRIVE guidelines 2.0. The UMICH Animal Welfare Assurance agreement is compliant with OLAW and USDA and is fully accredited by AAALAC International. This protocol was approved with the ID number PRO00010841. Male outbred Sprague Dawley rats from Charles River Laboratories, weighing 450 g and 15 weeks of age, were used.
1. Rat anesthesia
- Remove animals from their cage and place them in an anesthetic pre-operative induction gas chamber at 5% isoflurane and 100% oxygen at a flow rate of 0.8 to 1 L/min (vaporizer-controlled) to induce general anesthesia.
- Sedate rats in the anesthetic induction chamber, remove them from the chamber, weigh, lubricate their eyes with sterile ophthalmic ointment, and then place them in dorsal recumbency on a warm water circulating heating device. Confirm adequate depth of anesthesia using pedal reflex (firm toe pinch).
- Shave the ventral abdomen with electric clippers. Maintain general anesthesia at 2.5% isoflurane and 100% oxygen at 0.8 to 1 L/min with a non-rebreathing circuit through a nosecone.
2. Rat ultrasound scanning
- Monitor physiological assessments, including respiratory rate, heart rate, and temperature, during imaging.
- For abdominal imaging of the Inferior Vena Cava (IVC), apply conducting gel and orient the transducer in a transverse position. While presetting the peripheral vascular, use two-dimensional imaging mode or B-mode, lower the linear probe (10 MHz) on the center of the abdomen, adjusting depth with pressure until the abdominal vessels come into view.
- Differentiate IVC from the abdominal aorta by assessing compressibility and by assessing flow using both color and pulsed-wave Doppler mode with a high-frequency linear probe (10 mHz).
- When applying compression with the ultrasound probe, differentiate the two as the IVC is compressible, whereas the aorta maintains its shape and patency.
- Assess the direction and velocity of blood flow by using both color and pulsed-wave Doppler. The color Doppler window represents the flow toward the probe in red and flows away from the probe in blue. Switch the instrument to pulse-wave Doppler mode (Duplex mode) to assess blood flow direction and velocity over time. Acquire necessary flow images by using the ultrasound machine's automated image capture tool (The exact specifications for image acquisition may vary between ultrasound systems).
- Use the following assessment method: the aorta has blood flow toward the probe and a triphasic waveform, whereas the IVC has spontaneous flow away from the probe with a much lower amplitude.
- If the proximal IVC displays a normal waveform, yet a nonphasic or absent (flat) waveform is detected distally, explore the possibility of a venous obstruction between these points of examination.
- Once the IVC is located, identify the mid-section, which is in the middle third portion, inferior to the renal veins and superior to the IVC bifurcation, most likely where the lumbar veins are located.
- Measure at the mid-section IVC the wall-to-wall diameter in the transverse view using the cross-sectional B-mode image, recording the widest diameter of the vessel. Imaging acquisition may vary in different ultrasound machines. Store data using compact disks (CDs) in DICOM files.
3. Rat micro-surgery and recovery
- Clean the abdomen with gauze-soaked chlorhexidine scrub and chlorhexidine solution 3x to ensure an aseptic surgical condition.
- Place sterilized cling film as a surgical wrap to cover the rat thorax and abdominal area, microscope knobs (magnification and focus), and eyepiece.
- Make a ventral midline incision (3 cm) approximately 2 cm below the xiphoid process with iris scissors through the skin and abdominal wall, exposing the abdominal contents. Use sterile saline-soaked 2 inch x 2 inch gauze to reflect the intestines to the animal's right side.
- For IVC exposure, perform a blunt dissection using a sterile cotton-tipped applicator. Place a wire speculum in the incision, allowing IVC visualization.
- Cauterize all IVC lumbar branches using a low-temperature fine tip cautery, from the renal veins to the iliac bifurcation, and ligate side branches with 7-0 non-absorbable polypropylene sutures.
- Place a proximal curved vascular micro-clip on the IVC, which is separated from the aorta and just inferior to the renal veins. Place a straight microclip on the distal IVC, which is separated from the aorta and superior to the IVC bifurcation.
- Place an 8-0 nylon U stitch suture caudal to the left renal vein centered on the anterior surface of the IVC.
- Insert a 0.014 mm sharpened guidewire with the venoplasty balloon backloaded, retrograde to blood flow into the infrarenal IVC, caudal to the curved micro-clip.
- Advance the balloon into the mid-IVC using the Seldinger technique. Remove the sharpened guidewire and inflate the venoplasty balloon for 3 min with a 10% to 15% IVC overstretch using a 20 mL inflation syringe to generate positive pressure over a range of 0-30 Atm. Flush all systems with sterile saline before IVC canulation to avoid air embolism.
NOTE: A 2.8 mm IVC would undergo venoplasty to 3.22 mm (15% overstretch). The required inflation pressure to reach the desired overstretch is determined by the characteristics of the balloon and is available on the manufacturer's packaging. - Tighten the U stitch upon venoplasty balloon deflation and removal. Remove the micro-clips.
- Close the laparotomy site in a two-layer fashion. Use a 5-0 polyglactin absorbable synthetic suture in a continuous pattern to close both the abdominal wall and skin.
- Administer buprenorphine extended-release injectable suspension, 0.65 mg/kg subcutaneous (SC) post-operatively as an analgesic for rats since it does not interfere with the biomarker panels of inflammatory molecules for protein analysis.
- Recover rats in an individual cage, observe post-operatively (30 min) under a heating lamp (minimum distance – 24 inch away from the cage), and then return to their original housing units.
- For sham animals from each experimental group, perform only the dissection, without the IVC branches ligation, cauterization, and cannulation.
- For post-thrombotic conditions, place a proximal straight vascular micro-clip on the IVC, which is separated from the aorta, just inferior to the renal veins, for 24 h. Use the same dissection and closing techniques.
- Check for the ultrasound signs of IVC occlusion, which include the visualization of the IVC clip, confirmation of distal IVC without flow, and common iliac veins distended. Follow-up timepoints can be customized to fit the study's specifications.
- To observe the physiologic changes that are being modeled, select timepoints in the first 72 h for early thrombi formation and from 3 to 7 days postprocedural for later thrombi resolution. Later timepoints tested in this model include 7 to 28 days5,13.
- Use the techniques in steps 3.5-3.9 for post-thrombotic balloon venoplasty with the following caveats: A higher insufflator pressure might be required to achieve the desired overstretch since the IVC diameter increases in post-thrombotic conditions.
- Perform euthanasia under the recommendations set forth by the current American Veterinary Medical Association Guidelines on Euthanasia for rodents by performing two confirmatory methods (blood removal and vital organ removal) to ensure the animal will not revive.
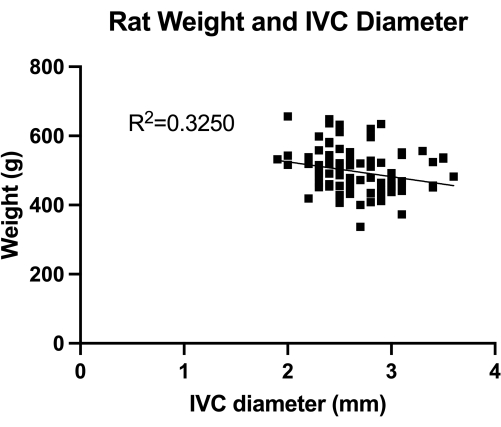
Figure 1: Distribution of transabdominal duplex measures of transverse IVC (mid-infrarenal section) diameter. The measurement was done by animal weight. No significant correlation was found between the weight and the IVC diameter. Please click here to view a larger version of this figure.
4. Sample preparation
- Perform confirmatory tissue transfer of drug-coated venoplasty balloons using high-performance liquid chromatography (HPLC) assay technique.
- Dissect the IVC and aorta and remove en bloc for formalin-fixed paraffin embedding and histological analysis.
- For protein analysis, use RIPA buffer in a diluting concentration of 60,000 µg/g of sample, process with a tissue homogenizer in low-temperature room settings at 4 °C, and store at -80 °C after processing.
The VBM is a model that evaluates the effect of venoplasty balloons in complete hemostasis control. First, we quantified the IVC (mid-infrarenal section) diameter, as shown in Figure 1, for correct balloon sizing. Second, the developed step-by-step microsurgical technique is illustrated in Figure 2, and we also show examples of the critical steps in Figure 3. Notice the retrograde approach used for the IVC canulation with the sharpened guide wire.
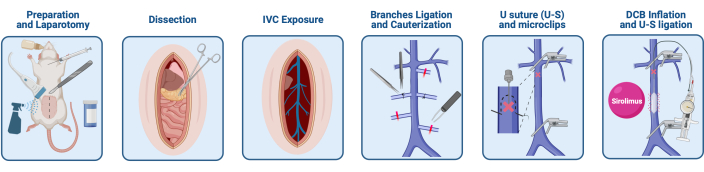
Figure 2: Microsurgical technique for the testing of venoplasty balloons in rats. The technique used is described here. Please click here to view a larger version of this figure.
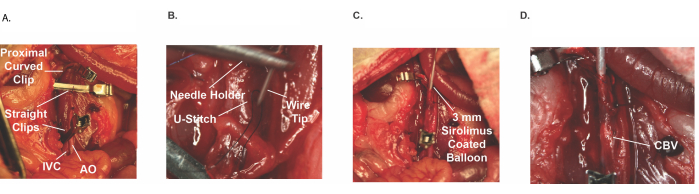
Figure 3: In vivo images of the deployment technique. (A) Hemostatic control. (B) U-stitch on infrarenal IVC. (C) Wire insertion through U-stitch with 3 mm sirolimus-coated balloon. (D) Balloon venoplasty retrograde deployment (Sirolimus coated). Abbreviations: IVC = inferior vena cava; AO = Aorta; CBV = Coated balloon venoplasty. Please click here to view a larger version of this figure.
Other normal venous vessel measurements and distinctions between the IVC and the aorta are highlighted in Figure 4. Thrombotic ultrasound findings are included in Figure 5. Finally, a comparison between the diameter of preoperative ultrasound and post-thrombotic measurements can be observed in Figure 6. Average pulsed-wave Doppler flow velocity (mm/s) in the inferior vena cava before and after clip placement of the vessel is shown in Figure 7.
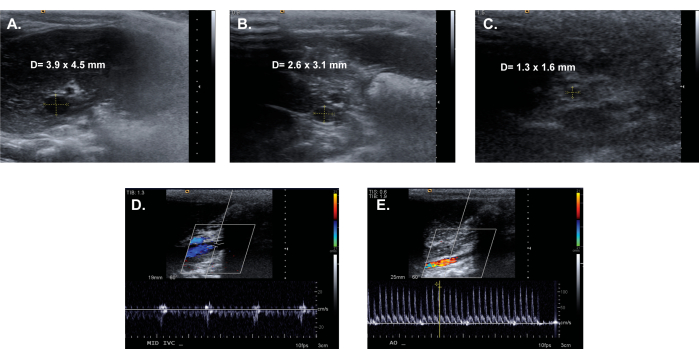
Figure 4: Representative transabdominal duplex images, with examples of a transverse IVC diameter calculation. (A) Proximal IVC. (B) Mid-infrarenal IVC. (C) Distal IVC. Color Doppler analysis of (D) Mid-infrarenal IVC and (E) Abdominal aorta. Please click here to view a larger version of this figure.
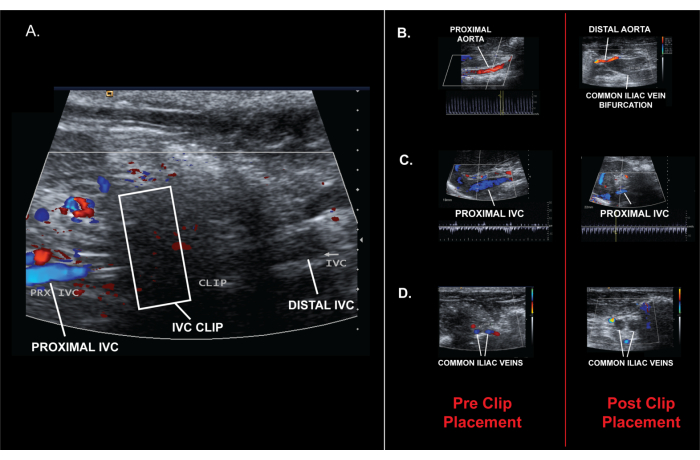
Figure 5. Images showing pre- and post-clip placement images. (A) Post clip placement ultrasound findings confirming IVC occlusion. (B) Proximal and distal aorta flow. (C) Proximal IVC flow. (D) Common iliac veins. Please click here to view a larger version of this figure.
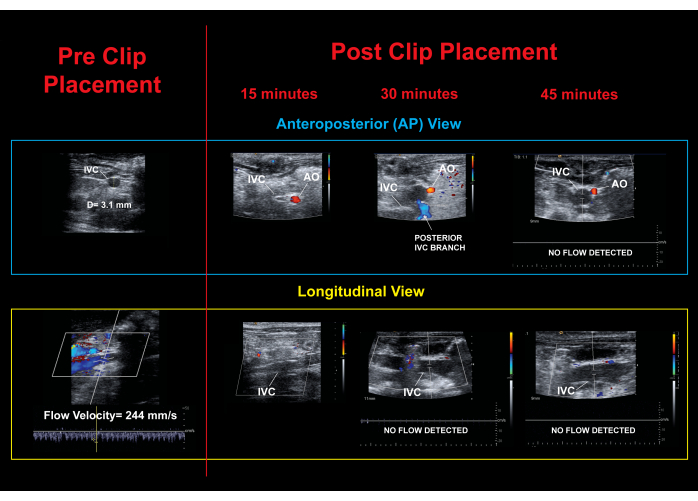
Figure 6. Ultrasound images. Ultrasound changes before and after 15 min, 30 min, and 45 min, confirming IVC occlusion. Please click here to view a larger version of this figure.
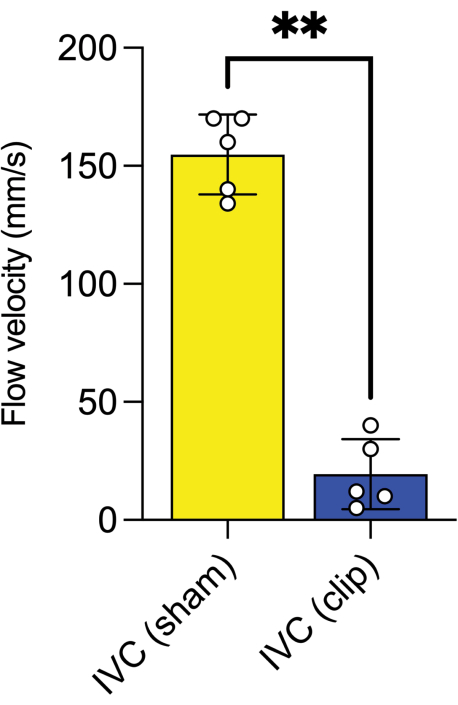
Figure 7: Average pulsed-wave Doppler flow velocity. Mean flow velocity (mm/s) in the inferior vena cava before and after clip placement (**: P ≤ 0.01, Mann-Whitney test performed). Error bars show standard error. Please click here to view a larger version of this figure.
To analyze the outcome of different venoplasty interventions with novel coatings, we recommend the measurement of effective proteins which can demonstrate the on-target effect of the drug of interest. For the sirolimus-coated venoplasty balloon used here, we measured phosphorylated AKT (p-AKT) protein levels of rat IVC lysates, confirming mTOR pathway inhibition since p-AKT is a downstream protein that decreases in response to sirolimus14,15. We can observe in Figure 8 how, after coated-balloon venoplasty (CBV), p-AKT is significantly decreased compared to the sham group.
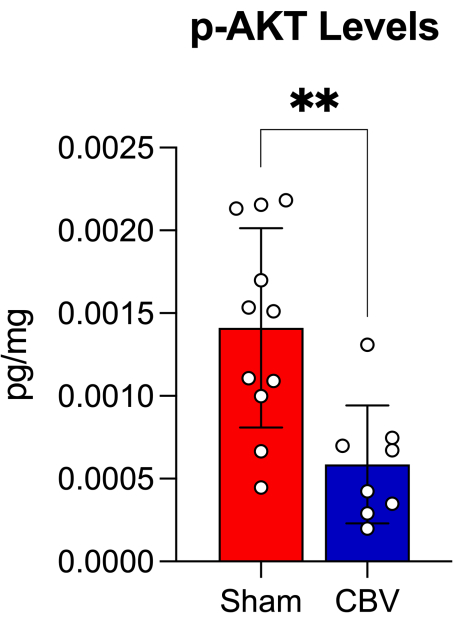
Figure 8: Protein p-AKT levels. Protein levels of rat IVC lysates of sham vs. coated-balloon venoplasty (CBV) in normal conditions confirming on target effect with mTOR pathway inhibition using sirolimus venoplasty coated balloons. (**: P ≤ 0.01, Mann-Whitney test performed). Error bars show standard error. Please click here to view a larger version of this figure.
