NOTE: The protocol described here is for BCG but can be applied to any Mycobacteria. BCG can be used as a surrogate bacterium for TB experiments when BSL3 facilities are not available22. The following procedures using BCG should be performed under a biosafety level 2 (BSL2) laboratory and follow the appropriate biosafety guidelines and good laboratory practices for the manipulation of hazard group 2 microorganisms.
1. Culture media preparation
- Prepare Middlebrook 7H9 broth supplemented with 10% (v/v) oleic acid, albumin, dextrose, and catalase (OADC) enrichment, according to the supplier's instructions. Supplement the broth with 0.05% (v/v) of tyloxapol.
NOTE: Tyloxapol is a non-ionic liquid polymer that has been used as a surfactant to prevent bacterial clump formation16. - Prepare Middlebrook 7H10 solid medium supplemented with 10% (v/v) OADC enrichment according to the supplier's instructions.
- Distribute 40 mL of medium per square Petri dish (120 mm x 120 mm). Allow the plates to dry to minimize condensation at the surface of the agar.
NOTE: This specific size of petri dish is fundamental to allow direct transposal of at least 96 droplets from a 96-well plate. Effective drying of the plates will later facilitate the plating of small droplets of bacterial suspension and prevent the droplets from spreading. - Prepare either Roswell Park Memorial Institute Medium (RPMI 1640) or Dulbecco's Modified Eagle Medium (DMEM) to produce the infection medium. In either case, supplement the medium with 10% fetal calf serum, 1% L-glutamine, and 1 mM sodium pyruvate. Do not add penicillin and streptomycin to the medium.
2. Sample preparation
- Obtain samples from a variety of sources. Typically, to quantify CFU to evaluate the efficacy of a TB vaccine, acquire samples from vaccinated and unvaccinated animal tissues. For example, mouse lung and spleen11 or macaque lung, thoracic and peripheral lymph nodes, spleen, liver, skin, blood, bone marrow, and bronchoalveolar lavage wash23. Alternatively, obtain samples from in vitro cultures of macrophages/dendritic cells/neutrophils infected with BCG18,19,20, 24,25,26.
3. Production of BCG culture
NOTE: For in vivo studies of TB vaccines, the aim is to improve the efficacy of BCG. Therefore, BCG-vaccinated groups are usually used as control. BCG strains used for human vaccination are ideal for testing in animal models. In this case, a culture of BCG must be reconstituted according to the supplier's instructions27. However, a BCG culture for in vivo studies can also be produced in-house11. The production of unicellular, uniform, and high-quality BCG culture for in vitro infection protocols has been produced very successfully in several studies11, 16, 18,19,20, 26, 28, 29, using the following protocol, which can also be used for animal challenge studies.
- Culture 50 mL of BCG in 7H9 broth, at 37 °C, with agitation at 200 rpm. Vary the volume according to the needs of the experiment.
- Every day, for 8-10 days, collect 100 µL of the culture and dilute it by adding 900 µL of PBS in a 1 mL cuvette. Then proceed by measuring the optical density of bacteria (OD at λ=600 nm; OD600) in a spectrophotometer. Draw a growth curve from those values. Identify the mid-log phase of the culture (when the OD is doubling consistently per unit of time).
- Prepare a subsequent culture and incubate until reaching the mid/late log growth phase as in steps 3.1 and 3.2. Use the values obtained in the previous step as guidance. Ensure that the culture does not reach the stationary growth phase (when the OD starts stabilizing) to maintain a good quality culture of viable bacteria.
- Collect the culture at the mid/late log growth phase. Centrifuge at 3000 x g for 10 min. Remove the supernatant.
- Add 10 mL of PBS to wash the bacteria. Centrifuge at 3000 x g for 10 min. Remove the supernatant.
- Resuspend the bacteria with 5 mL of infection media. Place the tube in an ultrasound bath for 15 min, full power at 80 Hz.
- Centrifuge at 1000 x g for 10 min. Collect the supernatant avoiding the pellet as it is rich in bacterial clumps that should be avoided in a high-quality BCG culture and discard it.
- Measure the OD of the supernatant. Here, cultures at the exponential growth phase, with an OD600 of 0.1, are equivalent to 1 x 107 CFU/mL.
NOTE: Each laboratory should produce its own BCG growth curves before starting experiments to establish a linear regression between OD600 and CFU using the spectrophotometer. Please note that spectrophotometers have different light path distances, which can vary the readings obtained for the same sample. - Carry out simple calculations to establish the number of bacteria to add to each host cell culture. The number of bacteria per host cell is the Multiplicity of Infection (MOI). Use an MOI of 10 bacteria per host cell, which is the most common MOI used for BCG infection experiments.
4. Micro-colony forming unit assay
NOTE: After an in vivo or in vitro infection experiment is completed, the enumeration of bacteria can be performed by mCFU. For in vivo studies, samples must be first homogenized in a bead beater or another tissue homogenizer. For in vitro cultures of macrophages/dendritic cells/neutrophils infected with BCG, samples must be lysed using a non-ionic detergent (e.g., 0.05% solution of non-ionic, non-denaturing detergent).
- Serial dilutions using a 96-well plate: perform serial 10-fold dilutions of the lysates, in a sterile 96-well plate according to the scheme in Figure 1A. Distribute the lysates on rows A and E. For each plate, the maximum number of samples and/or replicates is 24.
- Add 180 µL of dH2O to the remaining wells to perform the serial dilution.
- Using a 12-channel pipette, resuspend the lysates in row A and transfer 20 µL to row B (20 µL lysate + 180 µL dH2O). Homogenize well. Sequentially repeat this step for rows B and C until reaching the last dilution in row D.
NOTE: We usually perform three dilutions (100, 101, 102, 103), thus using 4 rows of the plate (A-D or E-H) for each set of 12 samples and/or replicates. - Micro droplet plating: use a 0.5-10 µL (thin tips are preferred) multichannel pipette to transfer 5 µL from each row of the 96-well plate to the solid medium square plate, according to Figure 1B.
- While slowly pipetting the 5 µL droplets, allow them to slightly touch the agar. This will help to take off the droplet from the tip towards the agar and reduce the possibility of retention of the liquid inside the tip.
- Allow the droplets to dry, close the agar plate, and incubate it at 37 °C while monitoring bacterial growth. Optionally, incubate the agar plates in a sealed plastic bag to prevent the plates from drying.
- Micro-colony counting: following approximately 6-10 days of incubation, check for individual colonies, visible to the naked eye (Figure 2).
- Count the colonies using the lowest magnification objective (4x or lower) of an inverted optical microscope or magnifying glass. Counts should be performed in the dilutions where the number of colonies is lower than 300 and higher than 30. Alternatively, use a camera to take a picture of the droplet to manually count colonies on the computer or use software such as ImageJ to automate colony counting.
- To express cell numbers in CFU/mL, use the following equation:

Where C = number of colonies counted, V = volume plated in µL, and Dil = dilution where the colonies were counted (100, 101, 102, 103). For example, if 30 colonies were counted in a 5 µL droplet in dilution 102, then:

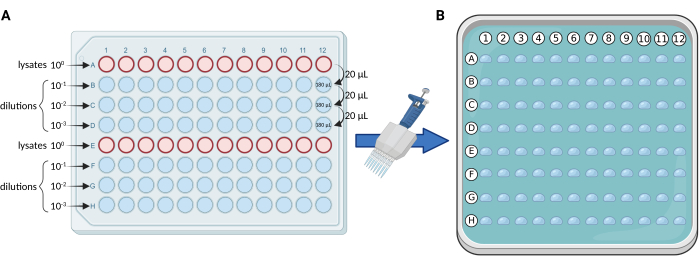
Figure 1. Schematic representation of the mCFU protocol. (A) Serial 10-fold dilutions of the BCG-containing lysates in a 96-well plate. (B) Square Petri dish containing solid culture medium and overlayed by 96 droplets of 5 µL each. Droplets are pipetted directly from the 96-well plate using a multichannel pipette. Created with BioRender.com. Please click here to view a larger version of this figure.
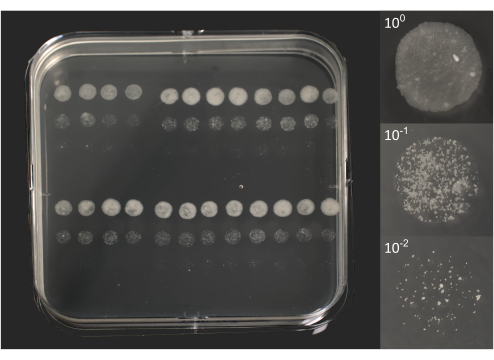
Figure 2. Micro-colony forming units of BCG following 10 days of incubation. On the left, a photo of a square Petri dish overlayed by 96 droplets of 5 µL each, as previously represented in Figure 1B. On the right, individual photos of 3 droplets correspond to an original lysate (100) and two dilutions (101, 102). Photos were taken using a DSRL camera equipped with an 18-55 mm zoom lens (plate) or a 105 mm macro lens (droplets). Please click here to view a larger version of this figure.
5. Micro-colony forming unit counting in Fiji (ImageJ)
NOTE: The mCFU method allows CFU quantification of large sets of samples. Pictures of the droplets may be recorded for posterior analysis to facilitate colony counting. Several photographic devices can produce images with sufficient quality for this purpose. These include digital cameras, webcams, camera-attached microscopes and magnifying glasses, and cell phones. Free image analysis software such as ImageJ offers the possibility of manual or automated colony counting in those images. To demonstrate both methods, Fiji will be used, which is a distribution of ImageJ that packages several tools for scientific image analysis30. Fiji can be downloaded from https://fiji.sc/.
- Manual counting method
- Open the image containing the mCFU in Fiji. Select Plugins > Analyze > Cell Counter.
- On the Cell Counter menu, select Initialize and then select a counter (e.g., Type 1).
- Proceed by clicking on each colony. Each click will be shown on the picture and will update the counter (Figure 3). To undo accidental clicks, select Delete.
- Register the value displayed on the counter. Click the Reset button to reset the count and open a new image to count additional samples.
NOTE: Further instructions on this plugin can be found at https://imagej.net/plugins/cell-counter.
- Automated counting method
- Open the image containing the mCFU in Fiji. Select Image > Type > 8 -bit. This will convert the image to an 8-bit gray-scale image.
- Select the Oval tool in the tool bar and draw an oval around the area with the colonies (Figure 4A). The oval may be adjusted after being drawn.
- Select Edit > Clear Outside, to remove any interference from the outside area (Figure 4B). Select Image > Adjust > Threshold.
- Move the sliders in the threshold menu until the colonies appear in red and background noise is minimized (Figure 4C).
- Select Apply and exit the threshold window. A black-and-white image is generated (Figure 4D).
- Select Analyze > Analyze Particles. In the analyze particles window, specify the range for colony area (between 1 and infinity, measured in squared pixels) and circularity (between 0 and 1, where 1 is a perfect circle; Figure 4E).
- Select Outlines in the show popup menu. Check Display Results for detailed measurements for each colony in the results window. Check Clear Results to erase any previous measurements. Check the Summarize box to display the summarized results of the measurements (Figure 4E).
- Initiate the analyzer by selecting OK. A new window appears, displaying all the outlined colonies that were detected and counted. The results window displays the details for each colony, and the summarized results window shows the total colonies counted (Figure 4F).
NOTE: The settings for size and circularity will vary with the image's resolution and magnification and the colonies' size and shape. Repeat the process several times until the best settings are found that detect all colonies. Further instructions on the analyze particles plugin can be found at https://imagej.nih.gov/ij/docs/menus/analyze.html#ap.
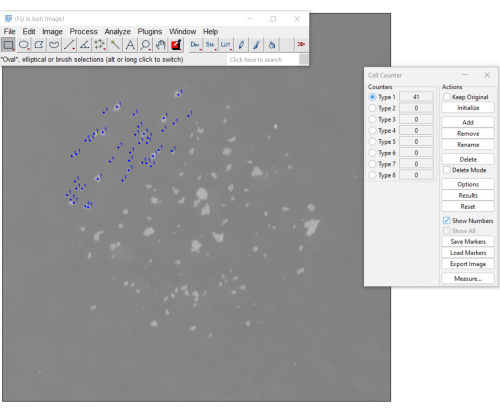
Figure 3. A manual method for counting mCFU using the cell counter plugin on Fiji software. The blue dots indicate colonies already clicked on by the user. The menu on the right displays the number of colonies counted so far (the count is 41). Please click here to view a larger version of this figure.
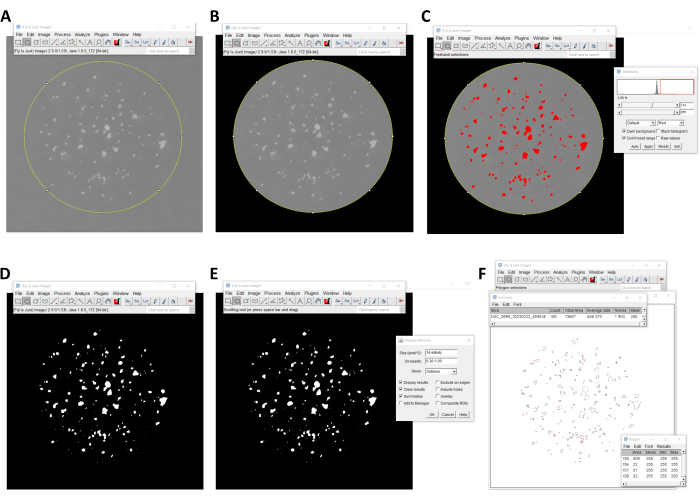
Figure 4. An automated method for counting mCFU using Fiji software. (A, B) The region of interest with the colonies is selected using the oval selection tool, and the outside area is removed using the clear outside command. (C, D) A black-and-white image of the colonies is generated using the threshold tool. (E, F) The number of colonies is quantified using the analyze particles tool. Please click here to view a larger version of this figure.
The mCFU assay described here increases the amount of information that can be retrieved from a single Petri dish to at least 96-fold. Figure 5 depicts a comparison of two drug-delivery methods for the repurposed use of saquinavir (SQV)31,32 as a host-directed drug to treat tuberculosis. In this assay, four different strains of Mycobacterium tuberculosis were used to infect primary human macrophages. M. tuberculosis H37Rv laboratory strain and three clinical strains isolated from patients with active TB by the Portuguese National Institute of Health's Dr. Ricardo Jorge (INSA): a drug-susceptible strain (INSA code 33427), a multiple drug-resistant (MDR) strain (INSA code 34192), and an extensively drug-resistant (XDR) strain (INSA code 163761). Each infection by each strain was further multiplied into eight different treatment conditions comparing three different concentrations of free-drug or liposome-loaded drug to the respective non-treated controls. Finally, each condition was analyzed at four different time points post-infection. To quantify intracellular bacterial growth, the total amount of lysates extracted from each time point was 32. This was followed by three serial dilutions to each lysate increasing the number to 128 samples. Multiplied by the four-time points analyzed results in 512 samples. Since the experiment was repeated using macrophages from at least three different blood donors, the total number of analyzed samples increased to 1536. Using the mCFU method described here, this experiment accounted for only 16 square Petri dishes versus 1536 that would be necessary using the standard CFU protocol. As shown in Figure 5, the results obtained with this method can demonstrate statistically significant differences between treatments.
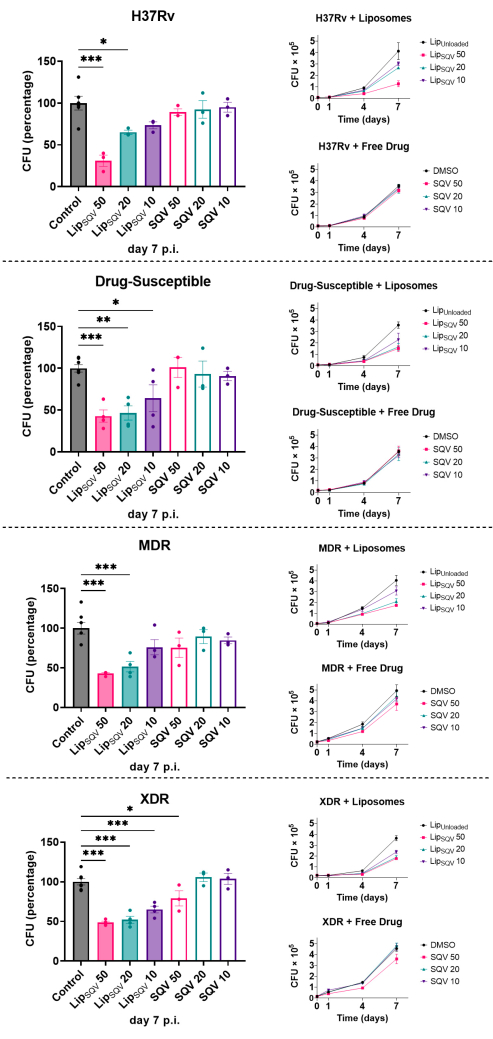
Figure 5. The mCFU method can produce high amounts of data from a small number of agar plates. This set of experiments tested the efficacy of the drug saquinavir (SQV) to induce intracellular killing of M.tb laboratory and clinical strains in human macrophages. SQV was administered to the macrophage cultures in its free form or loaded in liposomes (LipSQV). The treatments were performed in three different concentrations: 50, 20, and 10 µg/mL. Macrophages were infected with different M.tb strains for 3 h and then treated with selected concentrations of LipSQV and free SQV. Liposomes without the drug (LipUnloaded) and DMSO were used as controls. To evaluate bacterial intracellular survival, at discrete time points, macrophages were lysed, and serial dilutions of the bacterial suspension were plated on 7H10 agar plates. mCFU units were counted following 2-3 weeks. Lines depict the average mCFU per sample from at least 3 independent experiments. Bars represent the average mCFU percentage calculated relative to the respective controls at day 7 post-infection. Symbols represent each experiment with macrophages from a different donor. Error bars represent the standard error of the mean. Multiple group comparisons were performed using one-way ANOVA followed by a Holm-Sidak post-hoc test. * p ≤0.05, ** p ≤0.01, *** p ≤0.001. This figure has been modified from33. Please click here to view a larger version of this figure.
