The instrumented pull test (Figure 1) was used to investigate trunk and step responses in a young, healthy cohort23. Thirty-five trials were presented serially, with an auditory stimulus delivered concurrently with each pull (Figure 2). The auditory stimulus was either 90 dB (normal) or 116 dB (loud). The loud stimulus has been demonstrated as sufficient to trigger StartReact effects, where pre-prepared responses are released early by a startling auditory stimulus25. StartReact effects can be used as a probe to explore mechanisms underlying motor preparation26. The first-trial was kept to analyze unhabituated responses, and four subsequent trials discarded to allow for practice effects, which have been shown to habituate over five initial trials27. Subsequent habituated trials comprised 20 normal-intensity and 10 loud trials randomly intermixed. Inter-trial intervals (10 – 15 s) were variable. The analysis was conducted using linear mixed models due to multiple contributing factors that could influence trunk and step postural responses (e.g., variability of pull force between trials or participant height and weight). Linear mixed models' analysis was conducted using the following equation:

where Yij is the participant's reaction time or response magnitude for trial i, β0-5 are the fixed effect coefficients, θ0j is the random effect for participant j (random intercept), εij and is the error term.
The instrumented pull test distinguished first-trial responses and StartReact effects to a backward perturbation. During the first-trial, step reaction time was slower (first-trial vs. subsequent trials mean difference: 36.9 ms, p = 0.009), and stepping size was larger (first-trial vs. subsequent trials mean difference: 60 mm, p = 0.002) (Table 1). Trunk reaction time and response magnitude remained unchanged. StartReact effects were only present in the trunk to subsequent habituated pulls. A loud auditory stimulus accelerated truncal reaction time (loud vs. normal stimuli mean difference: 10.2 ms, p = 0.002) and increased truncal response magnitude (loud vs. normal stimuli mean difference: 588 mm.s-2, p < 0.001) (Figure 3 and Table 2). Variables contributing to the pull test responses were explored. Notably, examiner peak pull force was found to influence the size of stepping responses (p < 0.001) and trunk reaction times (p < 0.001) (Tables 3 and 4). Participant weight influenced step reaction times (p = 0.008) (Table 3). Otherwise, participant height and weight did not influence results.
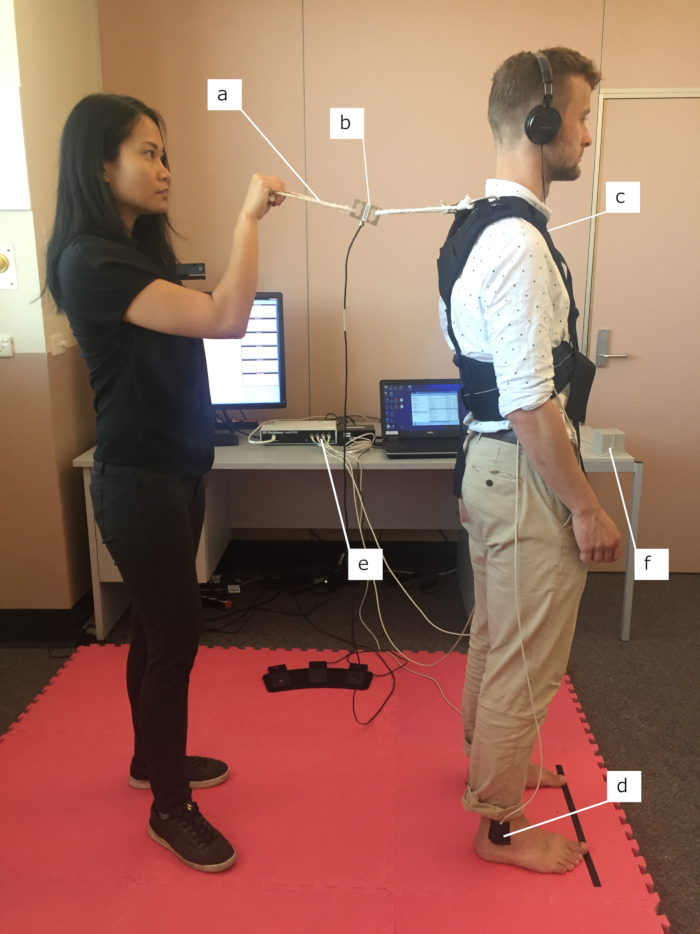
Figure 1. Set up of instrumented pull test. The instrumented pull test allows an assessor to apply a shoulder-level backward perturbation using a rope and harness (a). The force of the perturbation is recorded using a force gauge (b); the truncal response via a sensor placed at the sternal notch (c); and stepping via sensors on the left and right ankle malleolus (d). The motion tracking system encompasses a processing unit (e) which calculates three-dimensional positions of up to four sensors with respect to an electromagnetic transmitter (f). Auditory stimuli are delivered via headphones.This figure has been modified from23. Please click here to view a larger version of this figure.
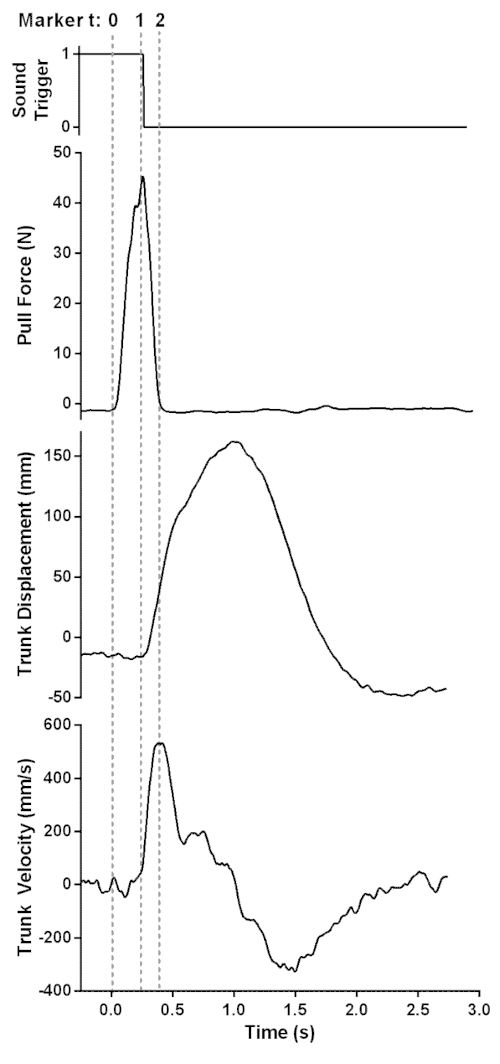
Figure 2. Data collected from a representative trial from the instrumented pull test. Vertical broken lines indicate markers on the time (t) axis. The onset of pull occurs at marker 0 with subsequent onset of trunk displacement at marker 1. Positive truncal displacement indicates backward movement. The auditory stimulus begins at the falling edge of the sound trigger, within 21 ± 6 ms of peak pull force. The onset of trunk deceleration at marker 2 occurs at the reversal of peak trunk velocity. The postural response (i.e., truncal reaction time) is defined as the difference between markers 2 and 1..This figure has been modified from23. Please click here to view a larger version of this figure.
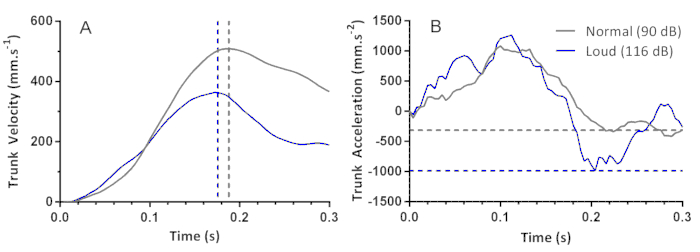
Figure 3. StartReact effects in truncal postural responses. Raw data representative of single trials associated with the normal stimulus at 90 dB (normal), indicated by the grey lines and loud auditory stimulus at 116 dB (loud), indicated by the blue lines. Vertical broken lines indicate markers on the time axis. StartReact is demonstrated by quicker reaction times in trunk velocity to the loud auditory stimulus, indicated by the blue broken vertical line, compared with the normal auditory stimulus, indicated by grey broken vertical line (A). Response magnitude to the postural task is derived from trunk acceleration. Horizontal broken lines indicate markers on the trunk acceleration axis. The largest response magnitude is shown in the loud trial, as indicated by the blue broken horizontal line representing the minimum point of the acceleration curve, compared to the normal trial, represented by the grey broken horizontal line (B). This figure has been modified from23. Please click here to view a larger version of this figure.
| Step Reaction Time | Step Response Magnitude | |||||
| Trial Type Comparison | Mean Δ (ms) |
95% CI | p-value | Mean Δ (mm.s-2) | 95% CI | p-value |
| First vs. Normal | 36.9 | 4.7, 69.2 | 0.009 | 60 | 17, 103 | 0.002 |
| First vs. Loud | 46.1 | 13.1, 79.2 | 0.002 | 53 | 9, 97 | 0.005 |
| Normal vs. Loud | 9.2 | -3.1, 21.5 | 0.072 | -7 | -23, 9 | 0.315 |
Table 1. Mean differences (Δ) between the first pull test trial and subsequent trials with 90 dB (normal) or 116 dB (loud) auditory stimuli for step reaction time and response magnitude.This table has been modified from23.
| Trunk Reaction Time | Trunk Response Magnitude | |||||
| Trial Type Comparison | Mean Δ (ms) |
95% CI | p-value | Mean Δ (mm.s-2) | 95% CI | p-value |
| First vs. Normal | -6 | -31.1, 19.0 | 0.692 | 162 | -412, 737 | 0.497 |
| First vs. Loud | 4.2 | -21.2, 29.6 | 0.692 | -425 | -1008, 158 | 0.12 |
| Normal vs. Loud | 10.2 | 3.0, 17.5 | 0.002 | -588 | -750, -425 | < 0.001 |
Table 2. Mean differences (Δ) between the first pull test trial and subsequent trials with 90 dB (normal) or 116 dB (loud) auditory stimuli for trunk reaction time and response magnitude.This table has been modified from23.
| Step Reaction Time | Step Response Magnitude | |||||
| Predictor | Estimate | 95% CI | p-value | Estimate | 95% CI | p-value |
| Peak Force | -0.12 | -0.44, 0.19 | 0.436 | 1.02 | 0.55, 1.49 | < 0.001 |
| Force Rate | -0.01 | -0.04, 0.02 | 0.575 | 0.01 | -0.03, 0.06 | 0.528 |
| Height | -64.65 | -283.98, 154.69 | 0.542 | 240.26 | -797.51, 1278.03 | 0.629 |
| Weight | 2.37 | 0.72, 4.03 | 0.008 | -2.51 | -10.56, 5.55 | 0.518 |
Table 3. Coefficient estimates, 95% confidence intervals (CI), and statistical significance of instrumented pull test predictors resulting from linear mixed models for step response.This table has been modified from23.
| Trunk Reaction Time | Trunk Response Magnitude | |||||
| Predictor | Estimate | 95% CI | p-value | Estimate | 95% CI | p-value |
| Peak Force | 0.36 | 0.22, 0.51 | < 0.001 | 0.98 | -2.95, 4.91 | 0.623 |
| Force Rate | -0.01 | -0.03, 0.00 | 0.062 | -0.12 | -0.47, 0.22 | 0.486 |
| Height | 45.97 | -31.16, 123.11 | 0.233 | -708.94 | -3362.70, 1944.82 | 0.587 |
| Weight | -0.17 | -0.75, 0.42 | 0.566 | 2.08 | -18.04, 22.19 | 0.834 |
Table 4. Coefficient estimates, 95% confidence intervals (CI), and statistical significance of instrumented pull test predictors resulting from linear mixed models for the truncal response.This table has been modified from23.
Supplementary Coding File. Please click here to download this file.
