The described protocol was implemented in a clinical setting at the China Medical University Hospital of Taiwan, and its feasibility and outcomes were assessed in a recently published clinical study25. The study enrolled a total of 31 participants (10 males, 21 females) to complete the intervention. The FSN group consisted of 15 participants (4 males, 11 females, mean age: 65.73 years ± 6.79 years), while the TENS group consisted of 16 participants (6 males, 10 females, mean age: 62.81 years ± 5.72 years) (Table 1). The results of the study showed that the FSN group exhibited a significant improvement in pain characteristics as measured by the VAS (p < 0.05) (Table 2). The study also revealed a significant difference in the PPT of the quadriceps muscle in the FSN group (p < 0.05), indicating an improvement in the muscle and tendon qualities, and this was particularly noticeable among the participants who received immediate treatment (Table 3). The functional index questionnaire assessment revealed that the FSN group demonstrated significant enhancements in the WOMAC and Lequesne index scores, reflecting improvements in physical function, pain, and stiffness. The improvements were noticeable in the immediate, 1 week, and 2 week follow-up periods (p < 0.05) (Table 4). The findings of this study provide evidence to support the feasibility of FSN therapy as a treatment option for patients suffering from painful knee OA. The results also establish the effectiveness of FSN treatment in alleviating the soft-tissue pain associated with knee OA caused by MTrPs (Figure 5).
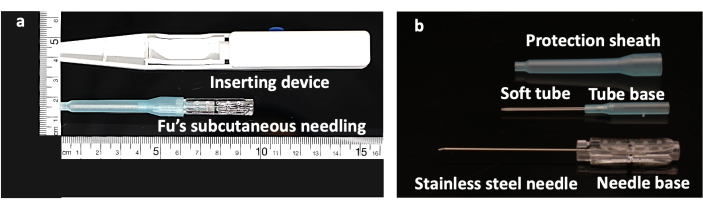
Figure 1: Structure of the Fu's subcutaneous needling needle. (A) FSN-inserting device with a FSN needle. (B) The FSN needle is made up of three parts: a solid steel needle core with a needle base (bottom), a soft tube (middle), and a protection sheath (top). Abbreviation: FSN = Fu's subcutaneous needling. Please click here to view a larger version of this figure.
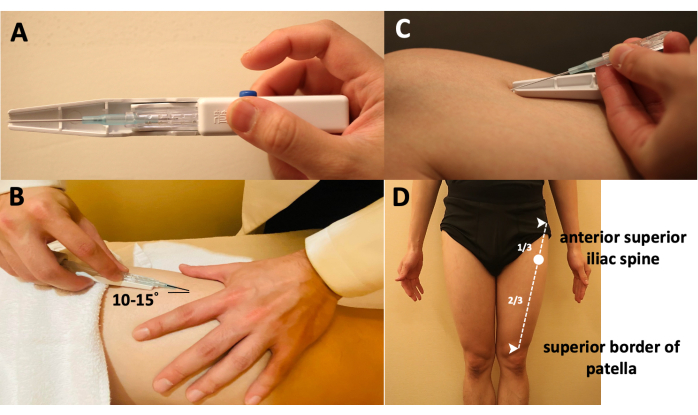
Figure 2: Manipulations of the Fu's subcutaneous needling needle. (A) The way of holding the inserting device. (B) The method to insert the FSN needle into the skin-the needle tip is placed at approximately 15° to the skin. (C) The method to separate the FSN needle from the inserting device. (D) Locating the insertion point, which is at the proximal one-third of the line from the anterior superior iliac spine to the superior border of the patella. Abbreviation: FSN = Fu's subcutaneous needling. Please click here to view a larger version of this figure.
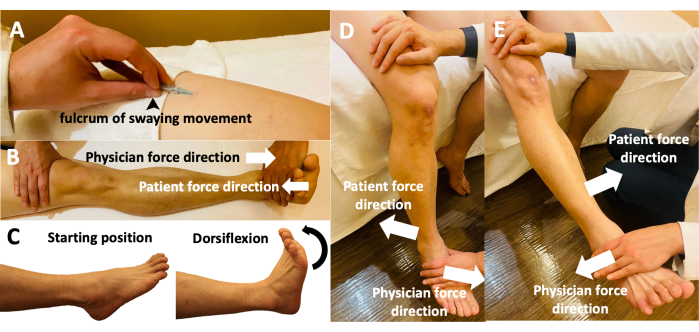
Figure 3: Fu's subcutaneous needling manipulations of the participants' limbs. (A) The holding of the FSN needle while performing the swaying movement. Using the thumb as the fulcrum, the middle finger and thumb affix the needle in a face-to-face manner, with the index and ring fingers moving back and forth. (B) Reperfusion approach with the participant performing a dorsiflexion movement and the physician performing an antagonistic movement with opposing dorsiflexion forces. (C) Reperfusion approach with the participant actively moving the relevant muscles and joints during dorsiflexion from the starting position. (D) Reperfusion approach with the participant actively performing knee flexion with the physician's resistance. (E) Reperfusion approach with the participant performing active knee extension against the physician's resistance. Abbreviation: FSN = Fu's subcutaneous needling. Please click here to view a larger version of this figure.
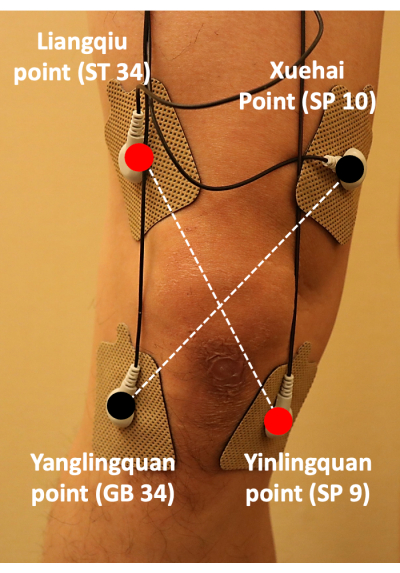
Figure 4: Positioning of the transcutaneous electrical nerve stimulation pads. TENS pads were attached at ST34, GB34, SP10, and SP9; the pads were placed in a cross pattern to treat the pain associated with knee osteoarthritis. Abbreviation: TENS = transcutaneous electrical nerve stimulation. Please click here to view a larger version of this figure.
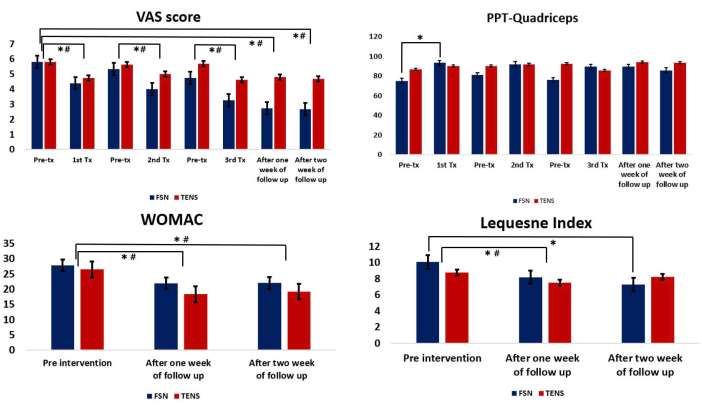
Figure 5: Comparison between the Fu's subcutaneous needling and transcutaneous electrical nerve stimulation groups. (A) The pre- and post-treatment values of the VAS. (B) The pre- and post-treatment values of the PPT for the quadriceps muscle. (C) Comparison of the WOMAC between the two groups after each treatment. (D) Comparison of the Lequesne index between the two groups after each treatment. * Represents the FSN group, p < 0.05; # represents the TENS group, p < 0.05. Abbreviations: VAS = visual analog scale; PPT = pressure pain threshold; WOMAC = Western Ontario and McMaster Universities Arthritis Index; Tx = treatment; FSN = Fu's subcutaneous needling; TENS = transcutaneous electrical nerve stimulation. Please click here to view a larger version of this figure.
Table 1: Baseline characteristics and clinical evaluation indicators of the participants. Data are expressed as mean ± SD; the P values were obtained from analyses with independent samples t-tests. This table is from Chiu et al.25. Abbreviations: FSN = Fu's subcutaneous needling; TENS = transcutaneous electrical nerve stimulation; VAS = visual analog scale; WOMAC = Western Ontario and McMaster Universities Osteoarthritis Index; PPT = pain pressure threshold; ROM = range of motion. Please click here to download this Table.
Table 2: Pain qualities compared between the FSN and TENS groups. Data are expressed as mean ± SD. This table is from Chiu et al.25. Abbreviations: FNS = Fu's subcutaneous needling; TENS = transcutaneous electrical nerve stimulations; VAS = visual analog scale; tx = treatment; F/U = follow-up. * Indicates a significant difference, as analyzed by a paired t-test. Please click here to download this Table.
Table 3: Muscle and tendon qualities (PPT of the quadriceps muscle) compared between the FSN and TENS groups. Data are expressed as mean ± SD. This table is from Chiu et al.25. Abbreviations: FNS = Fu's subcutaneous needling; TENS = transcutaneous electrical nerve stimulations; PPT = pain pressure threshold; tx = treatment; F/U = follow-up. * Indicates a significant difference, as analyzed by a paired t-test. Please click here to download this Table.
Table 4: WOMAC and Lequesne index compared between the FSN and TENS groups. Data are expressed as mean ± SD. This table is from Chiu et al.25. Abbreviations: FNS = Fu's subcutaneous needling; TENS = transcutaneous electrical nerve stimulations; WOMAC = Western Ontario and McMaster Universities Arthritis Index; tx = treatment; F/U = follow-up. * Indicates a significant difference, as analyzed by a paired t-test. Please click here to download this Table.
