To induce CA, the mouse was anesthetized with 1.5% isoflurane and ventilated with 100% nitrogen. This condition led to severe bradycardia in 45 s (Figure 1). Following 2 min of anoxia, the heart rate dramatically reduced (Figure 2), the blood pressure decreased below 20 mmHg, and the cerebral blood flow ceased completely (Figure 1). As the isoflurane was turned off, the body temperature was no longer managed and slowly dropped to about 32 °C at the end of CA (Figure 1).
Immediately following 8 min of CA, the ventilator was turned on, and the mouse was supplied with 100% oxygen. The blood-resuscitation mixture was infused into the circulation via the arterial catheter. Shortly after the injection of the blood-resuscitation mixture, cardiac function started to recover. After a short interval, the systemic and cerebral blood flow was restored, and ROSC was established. The success rate of ROSC is almost 100% in our lab. This model has been successfully performed in young and aged mice.
Enabled by this model, two imaging modalities were used in this study, including laser speckle contrast imaging (LSCI) and photoacoustic imaging, to monitor the cerebral blood flow and blood oxygenation at the whole-brain level during CA and resuscitation. LSCI confirmed the complete absence of blood flow in the brain during CA (Figure 3). More detailed changes in blood flow, structure, and oxygenation during the CA procedure can be obtained from the photoacoustic images (Figure 4).
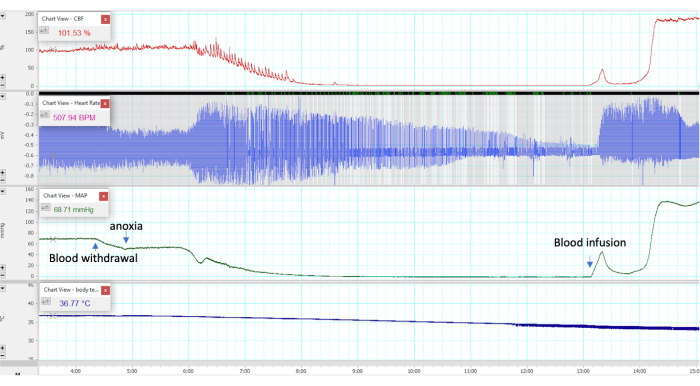
Figure 1: Physiologic recording during CA and resuscitation. Cerebral blood flow (% baseline; measured by laser Doppler flowmetry), blood pressure (mmHg), heart activity (beats per minute), and body temperature (°C) changes pre-CA, during CA, and after CA. The x-axis depicts the time in minutes. Please click here to view a larger version of this figure.
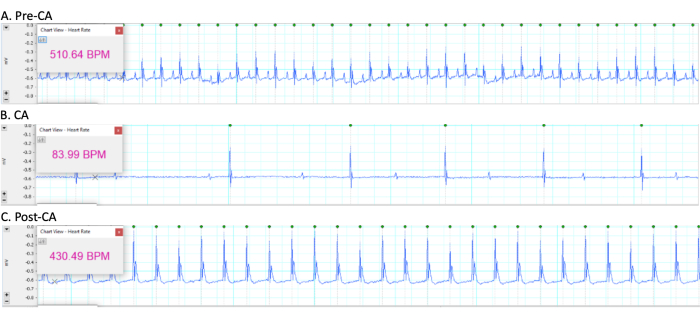
Figure 2: Heart activity during CA and resuscitation. The heart rate was continuously recorded, and panels (A), (B), and (C) are representative of the heart rate pre-CA, during CA, and post-CA, respectively. The y-axis depicts the absolute voltage values (mV). Please click here to view a larger version of this figure.
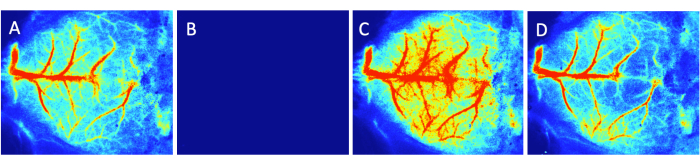
Figure 3: Laser speckle contrast images during CA and resuscitation. Global cerebral blood flow was monitored. CA led to a complete loss of cerebral blood flow (B) compared to baseline (A) . Hyperperfusion was present in the brain immediately after resuscitation (C) , and this was then followed by hypoperfusion during the late phase (D). Please click here to view a larger version of this figure.
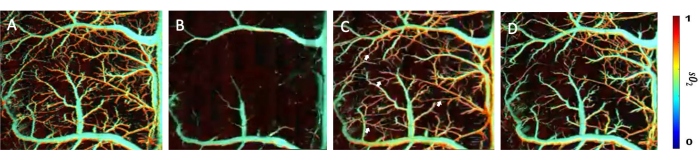
Figure 4: Photoacoustic images during CA and resuscitation. Local vascular changes were accessed using photoacoustic imaging. The arteries and branches were not perfused with blood during CA (B) compared to baseline (A) . All the arteries and branches were perfused immediately after resuscitation, including even some tiny bridges between branches (C, arrows). However, these bridges disappeared late (D) due to hypoperfusion. The bar shows the sO2 level. Please click here to view a larger version of this figure.
