By utilizing the information in the Description_Name field of DICOM files, the original MRI folder can be renamed to facilitate the rapid localization of the required imaging sequence during the analysis process in the imaging group. The MRI-IDEAL out-phase sequence is the type of MRI sequence used for providing clearer descriptions of liver tissue boundaries. This is because the MRI-IDEAL out-of-phase sequence can better differentiate the magnetization strength and angle of different tissues through specific image processing techniques.
The MRI-IDEAL out-phase sequence works by using gradient echo sequences (GREs) to generate images and utilizing out-phase control during image acquisition. This reduces the magnetic field inhomogeneity between tissues during imaging, thus improving the resolution and contrast of images for tissue structures. Additionally, the MRI-IDEAL out-phase sequence can also suppress the fat signal, thus reducing the interference of fat in imaging and providing a better display of adjacent tissue structures. In summary, the MRI-IDEAL out-phase sequence can improve imaging resolution and contrast by using techniques such as magnetic field control and fat signal suppression, resulting in clearer tissue boundaries.
Although deep learning tools can be used to extract the 3D anatomical structure of the liver, this method has a certain degree of machine learning error. The focus of this study is the precise quantification of hepatic fibrosis; therefore, the MIMICS tool was used for the extraction of the 3D liver tissue region, combined with expert experience to extract a relatively accurate 3D region of liver tissue.
The MRE stiffness map can display the shear stiffness of various spatial positions within each horizontal scan in the upper abdomen. This study focused on the early stages of hepatic fibrosis; therefore, the numerical range was 0-8 kPa. Figure 4 is the standard version of the MRE-Liver Stiffness Map on the GE device, which includes the stiffness map, but it is difficult to distinguish the liver's anatomical structure. The core innovation of this study is the precise quantification achieved by aligning the MRE-Liver Stiffness Map with the liver's anatomical structure shown in Figure 3.
Figure 5 provides an accurate stiffness map for the liver, which allows doctors and patients to have an exact understanding of the location and size of early hepatic fibrosis lesions, instead of a vague sense. This clears the way for further numerical quantification analysis.
Figure 6 is obtained by reconstructing the stiffness map of each liver scanned layer along the horizontal axis in 3D space; Figure 6 is the 3D version of Figure 5. In 3D space, the degree and location of a patient's hepatic fibrosis can be more clearly identified.
The results of comparing, analyzing, and studying pathological examination results with MRE stiffness can be found elsewhere9. To further quantify the numerical distribution of liver fibrosis stage in patients, Figure 7 lists the range of stiffness intervals for different stages used in this study based on previous research results.
According to the stiffness numerical range for different stages of liver fibrosis depicted in Figure 7, it is possible to calculate the specific proportion of liver 3D voxels in different stages for the patient. This calculation is based on the data from the 3D LSD as shown in Figure 6. Consequently, Figure 8 presents the quantitative results of the patient's hepatic fibrosis, indicating the proportion of the patient's liver that falls under different stages of hepatic fibrosis.
Based on the results shown in Figure 8, the data of a healthy liver were calculated as a comparison to illustrate the quantitative effect of the method researched in this study, as shown in Figure 9. The precise quantification difference between the two can be visualized. Based on this research paradigm, in subsequent studies, this group will conduct further investigation into the LSD of a healthy liver and the quantitative classification of early-stage hepatic fibrosis.
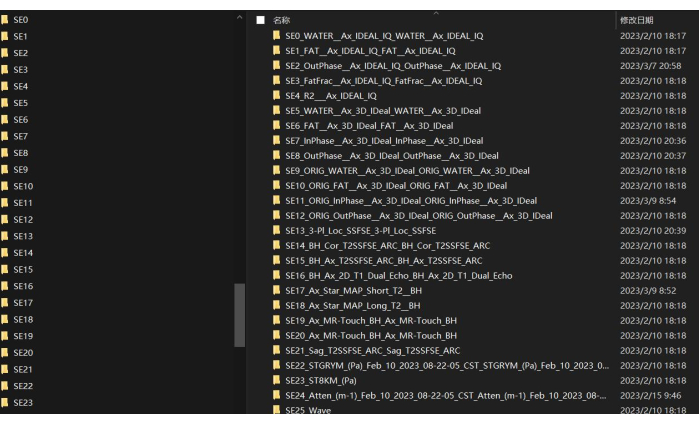
Figure 1: Description name of every MRI sequence. Shown here are the folder names of the MRI scan sequences. Please click here to view a larger version of this figure.
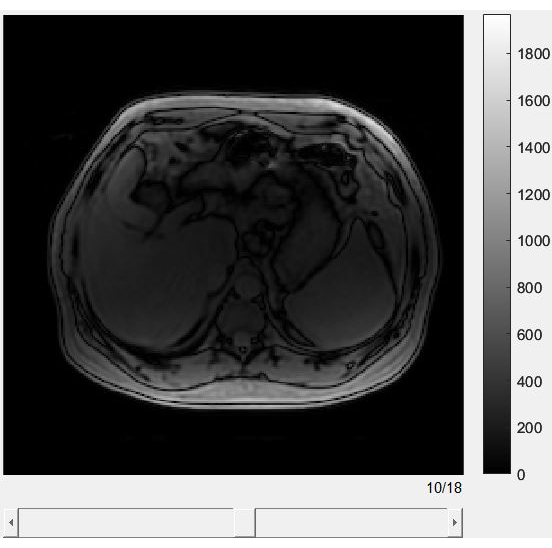
Figure 2: The graphic user interface of the slices of each IDEAL phase sequence. An example of browsing through MRI-IDEAL. MRI-IDEAL is a powerful tool that enhances the quality and interpretability of MRI images, particularly in cases where fat and water separation is critical. Please click here to view a larger version of this figure.
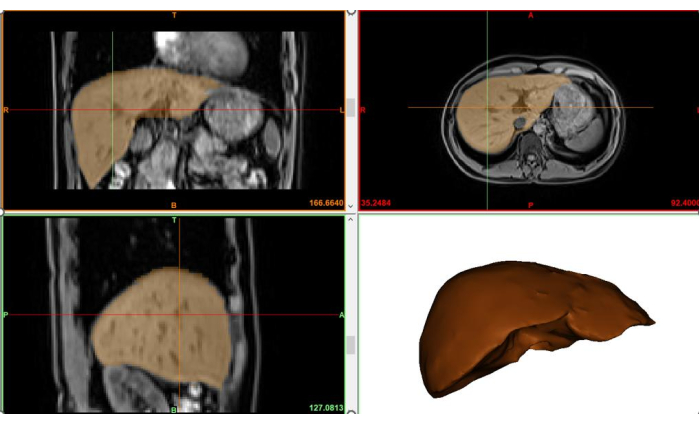
Figure 3: The extracted 3D region of the liver. Shows the 3D spatial extent of the liver based on structural images of the liver. Please click here to view a larger version of this figure.
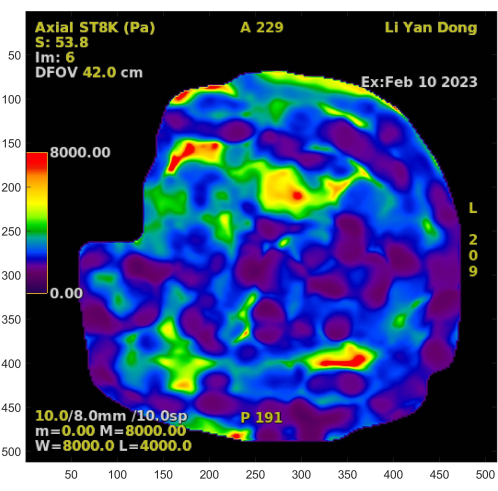
Figure 4: The Liver stiffness map. The standard version of the MRE-Liver Stiffness Map. Please click here to view a larger version of this figure.
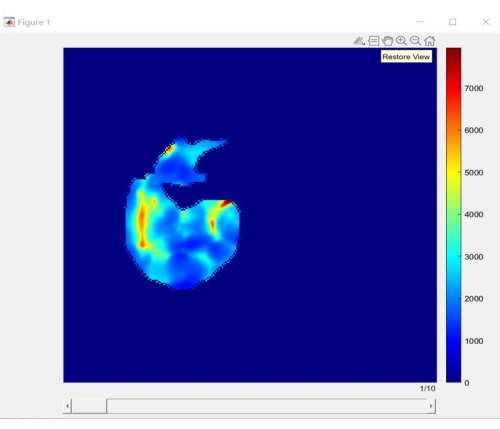
Figure 5: Slices of liver stiffness distribution. An accurate stiffness map belonging to the liver. Please click here to view a larger version of this figure.
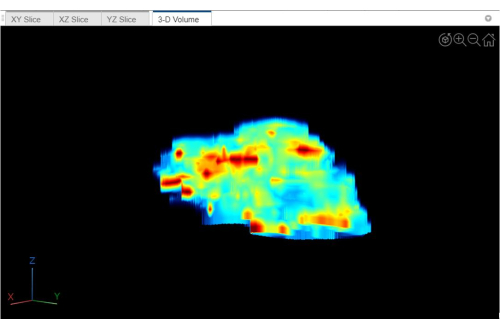
Figure 6: 3D-volume of liver stiffness distribution. This is the 3D version of Figure 5. Please click here to view a larger version of this figure.
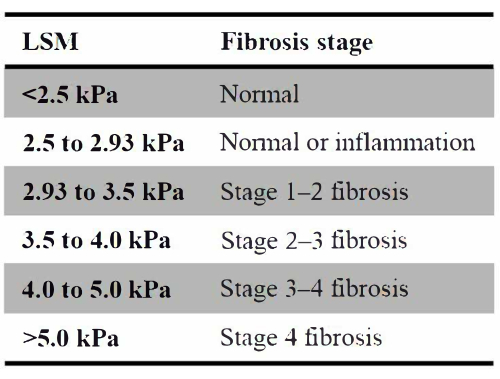
Figure 7: Different stages of hepatic fibrosis. List of the range of stiffness intervals for different stages used in this study based on previous research results. Please click here to view a larger version of this figure.
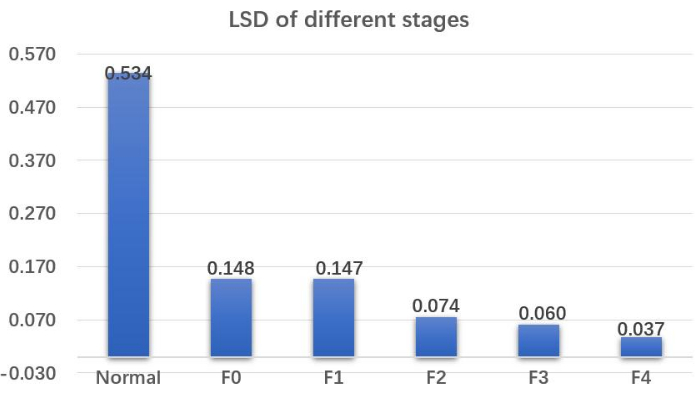
Figure 8: Liver stiffness distribution of the different stages. Quantitative results of the patient's hepatic fibrosis indicate the proportion of the patient's liver that falls under different stages of hepatic fibrosis. Abbreviation: LSD = liver stiffness distribution. Please click here to view a larger version of this figure.
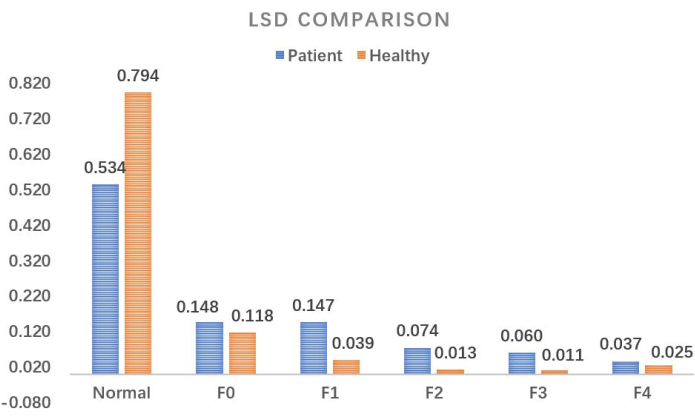
Figure 9: Comparison of liver stiffness distribution. A detailed quantitative comparison between a healthy liver and a patient with early-stage liver fibrosis. Abbreviation: LSD = liver stiffness distribution. Please click here to view a larger version of this figure.
