The efficacy of the method in inducing limbal stem cell deficiency (LSCD) was assessed by evaluating the clinical and histological signs of LSCD. Clinical assessment was done by slit-lamp microscopy and anterior segment- optical coherence tomography (AS-OCT) imaging (Figure 3 and Figure 4).
Re-epithelialization occurred in a centripetal manner and was faster at the temporal part of the cornea compared to its nasal part. Injured eyes developed 2+-3+ corneal haze immediately after chemical injury (Figure 3). Epithelial cells migrated from the conjunctiva to the corneal surface following limbal injury. The large corneal epithelial defect was re-epithelialized completely on days 12-14, which took longer compared to a corneal epithelial injuryof similar size and intact basement membrane and stroma which typically healed within 5 days post-injury8,9. Due to LSCD, 50% of the injured eyes developed persistent epithelial defects at the end of second week (Figure 3). Corneal edema was more prominent during the first few days (Figure 3, Figure 4), whereas corneal fibrosis was significant in the second week that resulted in 4+ corneal opacity in 100% of injured eyes.
Early signs of neovascularization (NV) were observed clinically and histologically, 24 h after chemical injury induction, as illustrated in Figure 5, consistent with the timeline of NV identified by Kvanta et al. study that showed sign of limbal NV 24 h after injury22. During the healing process, new vessels matured and by the 14th day after injury, NV crossed the limbus and reached the central cornea. The limbus, which defines the boundary between the conjunctiva and cornea, was destroyed.
Histological evidence of limbal stem cell deficiency and conjunctivalization were observed by the appearance of PAS+ goblet cells and stromal blood vessels23,24,25,26. Goblet cells were observed in the present injury model and indicated by the arrow in Figure 6.
Conjunctival and corneal epithelia principally express unique keratins, K13 and K12, respectively27. After the limbal injury, new epithelial cells that originated from the conjunctiva covered the denuded cornea, and K12 was not expressed on the corneal surface of any injured animals during 2 weeks after injury. This finding, consistent with other studies28, indicated complete LSCD and the absence of corneal epithelial cells on the corneal surface. However, in the study by Park et al.29, they detected K12 expression 20 and 32 weeks after injury, suggesting a possible trans-differentiation of the epithelial cells.
Consequently, we observed that chemical injury destroyed the limbus and limbal stem cells which resulted in the migration of conjunctival epithelial cells to the center of the cornea to cover the denuded corneal surface. This is further validated by the conjunctival epithelial cell marker, K13, which was expressed in the entire conjunctiva and corneal surfaces as shown in Figure 7.
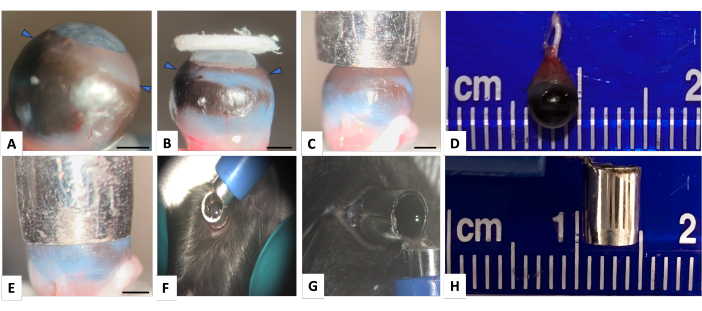
Figure 1: Normal mouse right eye and the punch-trephine for inducing corneal and limbal injury. (A) Lateral view showing mouse eye with highly curved cornea (arrowheads indicate the limbus). (B) The image demonstrates that even a large filter paper is insufficient to adequately cover the limbal area. The limbus-to-limbus diameter of the mouse eye is almost 4 mm and a punch biopsy with an external diameter of 4.5 mm and internal diameter of 3.5 mm (panels D and H), appropriately covers the cornea and limbal surface as shown in panels (C) and (E). (F) The punch-trephine is appropriately held over the globe around the limbal area. (G) To ensure that there is no leakage through the edge of the punch-trephine, after appropriately positioning the punch-trephine in a parallel axis with the globe, the hole is filled with methylene blue. No leakage of methylene blue is detected. Scale bar = 1 mm. Please click here to view a larger version of this figure.
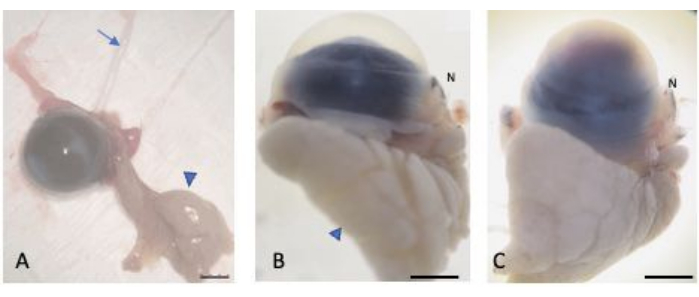
Figure 2: Enucleated eyes. (A) The eyes were enucleated while preserving the bulbar and palpebral conjunctiva, the lacrimal gland (arrowhead), and the optic nerve (arrow). The normal (B) and injured (C) eyes were saturated in 30% sucrose to protect against cryocrystal formation. The nasal part of the globe is recognizable through the nasal caruncle (labelled N). Scale bar = 1 mm. Please click here to view a larger version of this figure.
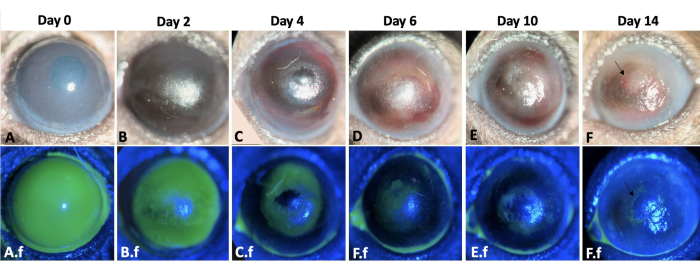
Figure 3: Wound healing of the left eye. The wound healing process of the left mouse eye throughout 2 weeks after corneal and limbal alkali injury in a mouse model is shown here (A-F). The slit lamp examination of the eye. Corneal edema is more prominent on days 0 and 2 (A,B), whereas fibrosis is more evident during the second-week post-injury (E-F). A.f-F.f show the re-epithelialization process of the same eye. Total corneal and limbal epithelial defect immediately after injury induction is observed in A.f. The epithelial defect healed by conjunctival epithelial cell migration in a centripetal pattern by 12-14 days (A.f-F.f). However, 50% of the injured eyes developed persistent epithelial defect at the end of second week as shown by arrow in F and F.f images. Scale bar = 1 mm (panel C). Please click here to view a larger version of this figure.

Figure 4: Anterior segment OCT of the mouse eye. (A) AS-OCT illustrates normal cornea curvature and anterior chamber. The iris structure is well-defined and recognizable. No iridocorneal adhesion is detectable at the mid-periphery of the iris. (B) Immediately after injury the corneal thickness increases due to edema formation and iridocorneal adhesion develops at the mid periphery of the iris. (C) Two weeks after injury the corneal curvature has changed and total iridocorneal adhesion with anterior chamber destruction is visible. Scale bar = 1 mm. Please click here to view a larger version of this figure.
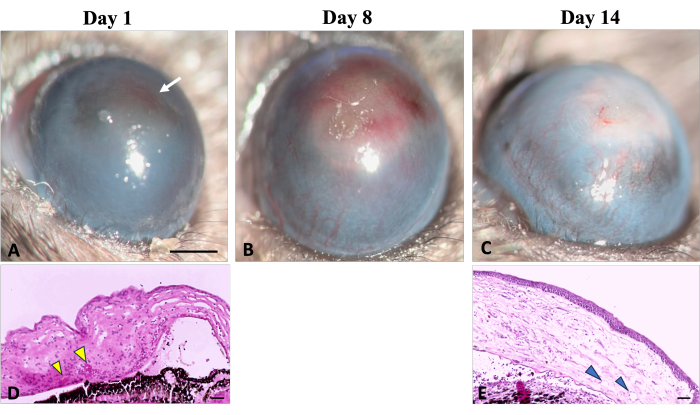
Figure 5: Corneal neovascularization. Clinical and histological signs of corneal neovascularization can be observed during the wound healing process following sodium hydroxide (NaOH) injury. (A) The initial signs of neovascularization become detectable on the first day after injury, characterized by a reddish discoloration of the cornea (indicated by a white arrow). This discoloration results from the aggregation of red blood cells in the stroma, as illustrated in corresponding histological image (D) (indicated by yellow arrowheads). (B) Over the first week of regeneration, new vessels progressively increase and spread throughout the cornea. (C) By the end of 2 weeks, the limbal area is destroyed, and the new vessels continue to evolve. (E) The histological section of the cornea further illustrates the presence of deep stromal neovascularization (shown by arrowheads). Slit lamp Image scale bar = 1 mm, the histology image scale bar = 50 µm. Please click here to view a larger version of this figure.
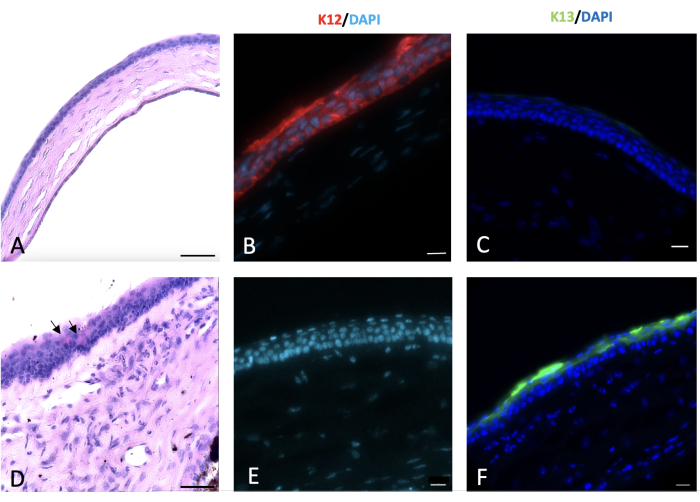
Figure 6: Periodic acid-Schiff and immunohistochemical (IHC) staining of cornea. Periodic acid-Schiff and immunohistochemical staining of the normal and injured cornea was done 2 weeks post-injury. Normal mouse corneal epithelium composed of 4-5 layers of cells (A). Alkali injury to the cornea and limbus led to conjunctivalization of the cornea with appearance of goblet cells on the corneal surface as shown by black arrows in (D). Normal corneal epithelial cells express K12 (B), which is not expressed by the conjunctival cells that cover the injured cornea (E). K13, a characteristic marker of conjunctival epithelial cells, is not expressed on the normal corneal epithelial cells (C). However, it is present on the sodium hydroxide (NaOH) injured corneal surface that is a sign of corneal conjunctivalization (F). Histology image scale bar = 50 µm, IHC stained image scale bar = 20 µm. Please click here to view a larger version of this figure.
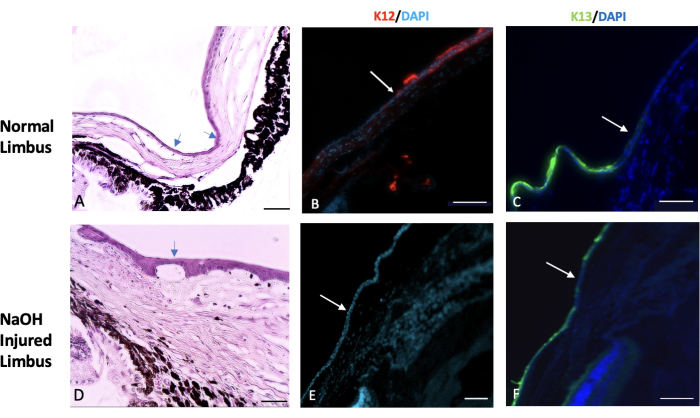
Figure 7: Hematoxylin and eosin and immunohistochemical staining. Hematoxylin and eosin (H&E) and immunohistochemical staining of the normal and injured limbus tissue was done. (A) The normal limbus marks the transition area between the end of the sclera and the beginning of the cornea. This region is typically covered by one or two layers of conjunctival epithelial cells (indicated by the arrows). In a healthy eye, the expression of a specific corneal epithelial marker called K12 begins at the limbus and extends to the surface of the cornea (shown in image B). On the other hand, the expression of a conjunctival marker known as K13 is restricted to the limbus and does not extend beyond it (indicated by the white arrow in image C). In eyes injured by sodium hydroxide (NaOH), the boundaries of the limbus are disrupted. This leads to migration of conjunctival cells towards the injured cornea. (D) The images of the NaOH-injured limbus demonstrate the presence of neovascularization both beneath the epithelial layer and within the stromal tissue. Following the injury, the injured corneal surface lacks the presence of K12 (E), while K13 is abundantly expressed on the corneal surface (F). Histology image scale bar = 50 µm, IHC stained image scale bar = 100 µm. Please click here to view a larger version of this figure.
Supplementary File 1: Staining protocol. Please click here to download this File.
Video 1: NaOH corneal and limbal injury in a mouse model with a punch-trephine. The video demonstrates the procedure of inducing NaOH corneal and limbal injury in a mouse model with a punch-trephine. It is crucial to hold the punch-trephine in a parallel axis with the globe and apply minimal pressure to the limbus. This proper technique is essential to prevent leakage and achieve optimal results. Please click here to download this Video.
Video 2: Illustration of the enucleation technique while preserving the bulbar conjunctiva. To differentiate the nasal side of the globe from the temporal side, the nasal caruncle is preserved along with the globe. The entire conjunctiva is dissected starting from its junction to the tarsal plate. With minimal pressure, the orbital contents protrude outward. By guiding the forceps toward the back of the globe, the optic nerve is grasped, and the tissue is extracted. The enucleated tissue includes the globe, orbital fat, and orbital lacrimal gland. Please click here to download this Video.
