Participants
From May 2022 to October 2022, a total of thirty healthy men and women were recruited to participate in the study. All participants had no history of cardiovascular, metabolic, or neurological diseases. They were not instructed to make any changes to their usual habits, including caffeine, alcohol, nicotine, vigorous exercise, or any other factors that could potentially impact vascular function.
Experimental procedures
Participants reported to the laboratory on two different experimental days 10 days apart. For each participant, the experiments were performed at the same time of the day, but the time of day differed between participants. Furthermore, the experiments were performed in the same room with limited light exposure, controlled temperature, no music, and limited conversation. On experimental day 1 and 2, the measurements were performed by the same sonographer (S1).
The participants were placed in the single-leg knee-extensor model described in the protocol and Supplementary Figure 1. The single-leg knee-extensor chair was constructed by a former professor at our research center (Professor Bengt Saltin), and is also referred to as the 'Saltin Chair' (see Table of Materials).
On two different experimental days, with a 10-day interval, participants reported to the laboratory. The experiments were conducted at the same time of day for each participant, although the specific time differed between participants. The experiments took place in a controlled environment, with limited light exposure, controlled temperature, no music, and limited conversation. On both experimental days (1 and 2), the measurements were performed by the same sonographer (S1). Participants were positioned in the single-leg knee-extensor model, as described in the protocol and Supplementary Figure 1. The single-leg knee-extensor chair, also known as the 'Saltin Chair' (see Table of Materials), was developed by Professor Bengt Saltin at our research center.
Initially, blood flow in the common femoral artery (CFA) of the dominant leg was measured in the seated resting condition, with the leg secured to the pedal. Subsequently, participants commenced the exercise, and blood flow was measured at the following workloads: 0 W, 6 W, 12 W, and 18 W. Each exercise session lasted for 4 min and was performed continuously. Two blood flow measurements were taken at each workload to ensure a steady state. The measurements were obtained at 2.5 min and 3.5 min into each workload21. To assess within-day reliability, the probe was briefly lifted away from the artery for 10 s after the first measurement, and then repositioned for the second measurement, as shown in Figure 1. The end-systolic diameter of the CFA, measured at rest, was used to calculate flow throughout the experiment.
On the third experimental day, the variation between the two sonographers was investigated using the same exercise protocol described above. Six participants provided informed consent for a third visit. Two skilled sonographers, experienced in measuring blood flow in clinical settings, performed measurements within 1 min of each other at the same workload, as depicted in Figure 1. Skilled sonographers were defined as having completed a minimum of 20 h of scanning volunteers in the single-leg knee-extensor model, including supervision for error correction. Both sonographers demonstrated comparable within-day reliability. During the exercise, the two sonographers measured blood flow in a randomized order, while being blinded to each other's measurements. To avoid audio and visual feedback, the sonographers were not present in the room simultaneously. The first sonographer completed the first measurement after 150 s at a given workload. After completing the trace, the first sonographer reset the ultrasound apparatus to default settings and left the room. The participant maintained the same pace and load, and then the second sonographer entered the room to obtain a new trace. Both sonographers performed blood flow measurements for the four workloads, as in experimental days 1 and 2. Prior to scanning at each workload, a coin flip determined the randomized order for the sonographers, ensuring that the 'winner' started the measurement. On experimental day 3, each sonographer obtained only one blood flow measurement during each exercise session.
统计学
All statistical analyses were conducted using statistical software. A significance level of p < 0.05 (two-tailed) was considered statistically significant. The data are presented as mean (standard deviation, SD) or mean [95% confidence interval, lower limit (LL), upper limit (UL)]. Paired t-tests were used to assess within-day and between-day differences in LBF. The p-values were Bonferroni corrected, with a threshold of 0.005 for statistical significance.
Reliability measures the amount of random error introduced by variability in the measured variable22. Absolute reliability was assessed using Bland-Altman plots and presented as limits of agreement (LOA) and smallest real difference (SRD), which estimate the expected difference between two measurements in 95% of cases23,24. One-way analysis of variance (ANOVA) was used to determine the standard deviation within participants (SDw), and SRD was calculated using the following formula24:

To compare the method with other LBF measurement techniques, the coefficient of variance (CV) was calculated as a relative measure of reliability. CV expresses the proportion of variance caused by measurement error25:
Based on the distribution of mean estimates and residual variance from a linear mixed model, the distribution of CV was simulated to obtain 95% confidence intervals for CV26. There is no official consensus on the quality levels of CV values, as they depend on the methodology and study type. However, CV is generally considered low if <10%, acceptable if 10%-20%, and non-acceptable if above 25%25,27.
In this study, sonographer 1 and sonographer 2 were the only raters of interest, and multiple measurements were performed to determine the appropriate ICC model to use. The intraclass correlation coefficient (ICC) was calculated using a two-way mixed-effects model with the absolute agreement and multiple measurements ICC (3, k). The first number refers to the model (1, 2, or 3), and the second number/letter refers to the type, indicating whether it is a single rater/measurement (1) or the mean of raters/measurements (k)28,29.
Both absolute and relative reliability are commonly used to assess the reliability of a measurement. Repeatability refers to the consistency of obtaining the same results when the measurement is repeated under identical conditions. Reproducibility, on the other hand, refers to the ability to obtain consistent results when the measurement is performed under varying or changing conditions. These terms are useful for understanding and evaluating the reliability of a measurement method22.
All participants successfully completed the study and tolerated the experimental design. A total of 30 healthy subjects (age: 33 ± 9.3, male/female: 14/16) were included, with a mean weight of 74.5 kg (SD: 13) and a mean height of 174 cm (SD: 9.3).
Absolute values and internal consistency
There were no statistically significant differences in the absolute LBF values between within-day or between-day measurements (Table 1). LBF increased progressively across the incremental workloads (Figure 2), ranging from 0.36 (SD: 0.20) L/min at rest to 2.44 (SD: 0.56) L/min during exercise at 18 W, demonstrating a linear increase with workload progression.
Bland-Altman plots illustrating LBF measurements are presented for within-day reliability in Figure 3, between-day reliability in Figure 4, and inter-rater reliability in Figure 5. Within-day data showed no outliers, while a few outliers were observed in the between-day measurements, and several outliers were observed during the inter-rater measurements.
Test-retest reliability
Values for smallest real difference (SRD), the coefficient of variation (CV), and intraclass correlation coefficient (ICC) are provided for within-day in Table 2, between-day in Table 3, and for inter-rater in Table 4.
The within-day SRD values ranged from 0.28 [95% CI: 0.22, 0.38] L/min during 0 W to 0.39 [95% CI: 0.32, 0.50] L/min during 18 W. The SRD values were higher in the between-day measurements ranging from 0.66 [95% CI: 0.41, 1.32] L/min at 0 W to 0.71 [95% CI: 0.53, 1.01] L/min during 18 W. The SRD was even higher in the inter-rater measurements ranging from 0.23 [95% CI: 0.12, 0.70] L/min at rest to 1.55 [95% CI: 1.02, 2.82] L/min during exercise at 18 W.
The CV values ranged from 4.0 [95% CI: 3.0, 5.1] % during 18 W to 4.2 [95% CI: 3.1, 5.3] % during 0 W. The CV was also higher in the between-day measurements ranging from 20.2 [95% CI: 14.7, 27.2] % during rest to 10.1 [95% CI: 7.5 to 13.1] % during 6 W. Even higher values were obtained during the inter-rater measurements with a CV ranging from 26.8 [95% CI: 11, 51] % at rest to 17.9 [95% CI: 8.5, 29.2] % during 6 W.
The ICC values showed that the reliability at all workloads, both during within-day and between-day, was >0.90. Conversely, the inter-rater measurements yielded ICC values as low as 0.41 (0.1 to 0.84).
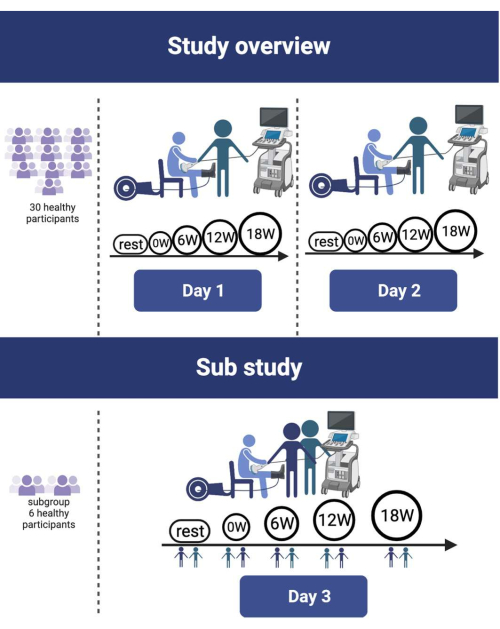
Figure 1: Study design overview. A total of 30 healthy participants underwent a single-leg knee-extensor protocol with incremental workloads ranging from 0 to 18 W. This protocol was repeated within a 10-day period. A subgroup of 6 participants volunteered for the inter-rater reliability study on day 3. Please click here to view a larger version of this figure.
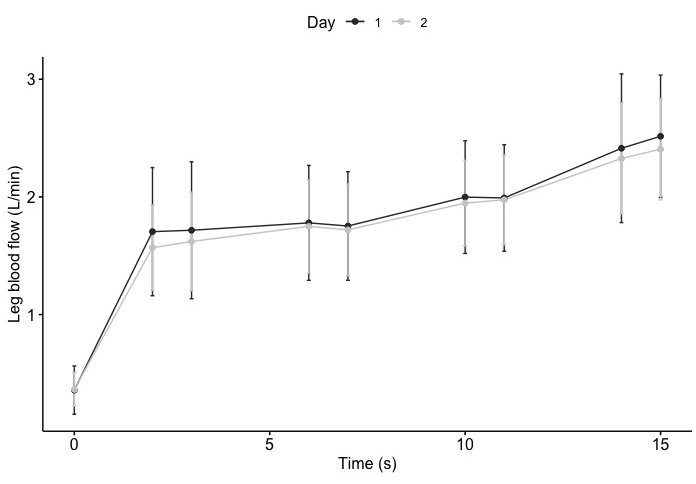
Figure 2: Leg blood flow response to single-leg knee-extensor exercise. The mean values for day 1 and day 2 are represented by black and grey dots, respectively, with whiskers indicating the standard deviation. One measurement was obtained at rest, and two measurements were obtained at each workload (0, 6, 12, and 18 W). Please click here to view a larger version of this figure.
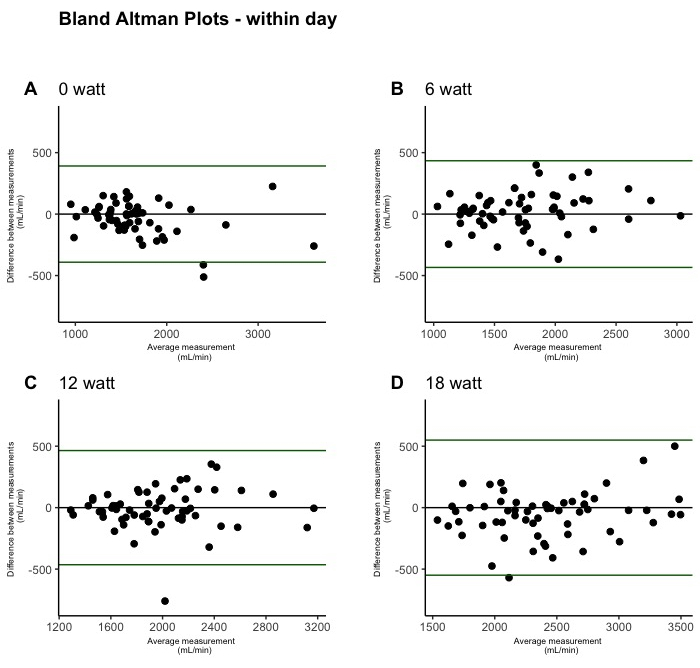
Figure 3: Within-day test-retest reliability of leg blood flow during single-leg knee-extension depicted by Bland-Altman plots. The plots were created from within-day measurements on both days (n = 60). One plot is shown for each incremental workload: 0 W (A), 6 W (B), 12 W (C), and 18 W (D). Please click here to view a larger version of this figure.
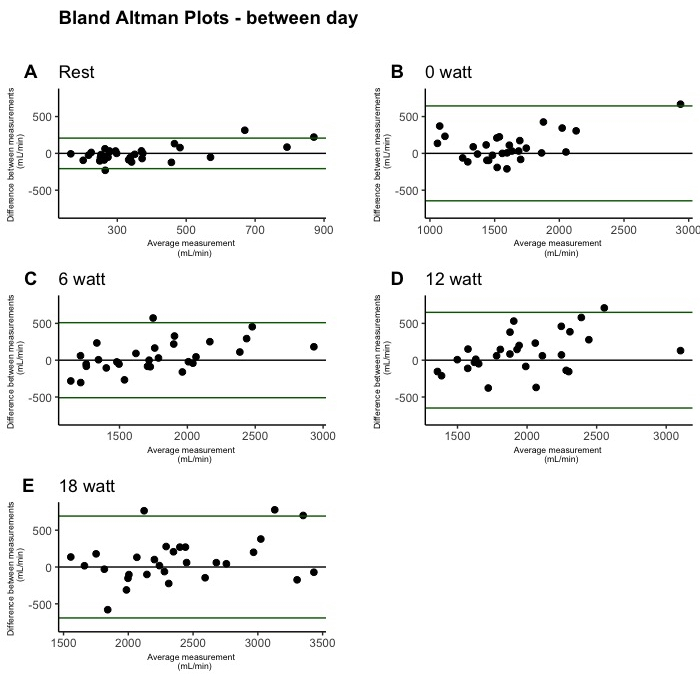
Figure 4: Between-day test-retest reliability of leg blood flow during single-leg knee-extension depicted by Bland-Altman plots. The plots were created from between-day measurements (n = 30). One plot is shown for each condition: rest (A), 0 W (B), 6 W (C), 12 W (D), and 18 W (E). Please click here to view a larger version of this figure.
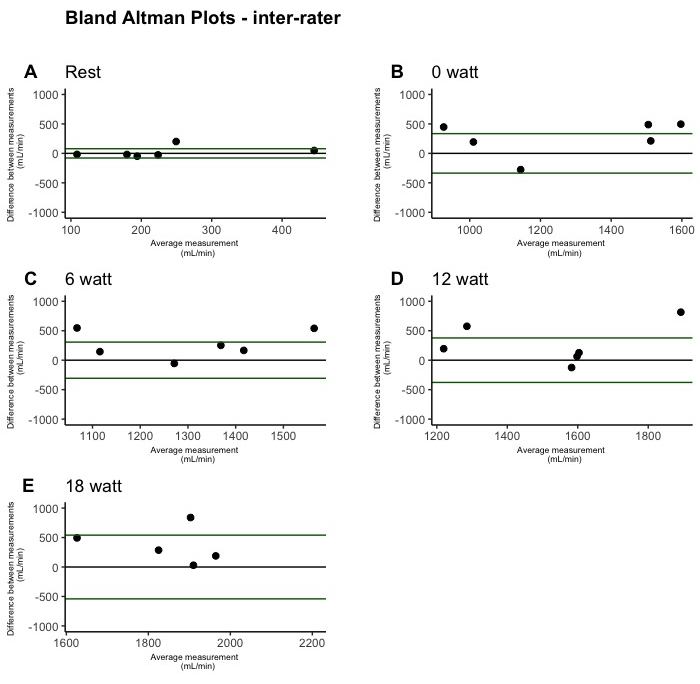
Figure 5: Inter-rater test-retest reliability of leg blood flow during single-leg knee-extension depicted by Bland-Altman plots. The plots were created from inter-rater measurements (n = 6). One plot is shown for each condition: rest (A), 0 W (B), 6 W (C), 12 W (D), and 18 W (E). Please click here to view a larger version of this figure.
| N = 30 | Day 1, 1. LBF | Day 1, 2. LBF | Within-day p-value | Day 2,1. LBF | Day 2,2. LBF | Within-day p-value | Between-day mean difference | Between-day | Day 1, CFA diameter (cm) | Day 2, CFA diameter (cm) |
| Rest (L/min) | 0.36 (0.20) | NA | NA | 0.37 (0.14) | NA | NA | 0.006 (0.11) | 0.76 | 0.94 (0.12) | 0.96 (0.14) |
| 0 W (L/min) | 1.68 (0.40) | 1.69 (0.47) | 0.60 | 1.58 (0.34) | 1.63 (0.40) | 0.03 | 0.13 (0.30) | 0.37 | ||
| 6 W (L/min) | 1.77 (0.45) | 1.75 (0.46) | 0.53 | 1.74 (0.40) | 1.72 (0.39) | 0.25 | 0.02 (0.26) | 0.37 | ||
| 12 W (L/min) | 1.99 (0.50) | 1.99 (0.45) | 0.8 | 1.95 (0.37) | 1.97 (0.38) | 0.42 | 0.07 (0.32) | 0.4 | ||
| 18 W (L/min) | 2.43 (0.55) | 2.51 (0.53) | 0.10 | 2.34 (0.44) | 2.38 (0.45) | 0.12 | 0.12 (0.33) | 0.06 |
Table 1: Leg blood flow. This table displays the absolute blood flow values and common femoral artery diameter measurements obtained on day 1 and day 2 during the first and second blood flow measurement. The data is presented as mean (standard deviation). A paired t-test was conducted to assess within-day and between-day differences. Abbreviations: W = watt, CFA = Common femoral artery. The p-value considered statistically significant after Bonferroni correction was set at p = 0.005.
| SRD (L) | CV (%) | ICC (Fraction) | |
| 0 W | 0.28 (0.21 to 0.38) | 4.2 (3.1 to 5.3) | 0.98 (0.96 to 0.99) |
| 6 W | 0.31 (0.26 to 0.38) | 4.3 (3.3 to 5.5) | 0.97 (0.95 to 0.99) |
| 12 W | 0.31 (0.24 to 0.50) | 4.1 (3.1 to 5.2) | 0.96 (0.93 to 0.97) |
| 18 W | 0.39 (0.32 to 0.50) | 4.0 (3 to 5.1) | 0.96 (0.94 to 0.98) |
Table 2: Within-day reliability measurements. The table presents the mean values (with 95% confidence intervals, lower limit, upper limit) for within-day reliability measurements. W = watt. SRD = Smallest real difference, CV = Coefficient of variance, ICC = Intraclass correlation coefficient.
| SRD (L) | CV (%) | ICC (Fraction) | |
| Rest | 0.21 (0.16 to 0.32) | 20.2 (14.7 to 27.2) | 0.92 (0.82 to 0.96) |
| 0 W | 0.66 (0.41 to 1.32) | 13.7 (10.3 to 17.6) | 0.93 (0.86 to 0.97) |
| 6 W | 0.52 (0.38 to 0.79) | 10.1 (7.5 to 13.1) | 0.91 (0.82 to 0.96) |
| 12 W | 0.66 (0.50 to 0.94) | 11.5 (8.6-14.7) | 0.82 (0.62 to 0.91) |
| 18 W | 0.71 (0.53 to 1.01) | 10.2 (7.6 to13.1) | 0.90 (0.79 to 0.95) |
Table 3: Between-day reliability measurements. The table provides the mean values (with 95% confidence intervals, lower limit, upper limit) for between-day reliability measurements. W = watt. SRD = Smallest real difference, CV = Coefficient of variance, ICC = Intraclass correlation coefficient.
| SRD (L) | CV (%) | ICC (Fraction) | |
| Rest | 0.23 (0.12 to 0.70) | 26.8 (11 to 51) | 0.85 (0.1 to 0.98) |
| 0 W | 0.96 (0.75 to 1.31) | 20 (9.2 to 33.3) | 0.74 (0,1 to 0.96) |
| 6 W | 0.88 (0.59 to 1.55) | 17.9 (8.5 to 29.2) | 0.6 (0.2 to 0.94) |
| 12 W | 1.09 (0.59 to 1.55) | 18.7 (8.8 to 30.6) | 0.5 (0.2 to 0.93) |
| 18 W | 1.55 (1.01 to 2.82) | 18.4 (8.6 to 30.1) | 0.41(0.1 to 0.84) |
Table 4: Inter-rater reliability measurements. The table presents the mean values (with 95% confidence intervals, lower limit, upper limit) for inter-rater reliability measurements. W = watt. SRD = Smallest real difference, CV = Coefficient of variance, ICC = Intraclass correlation coefficient.
Supplementary Figure 1: Single-leg knee-extensor model. This image depicts a participant during the trial while using the single-leg knee-extensor model. Prior consent was obtained from both the participant and the sonographer for the usage of this image. Text boxes are used to highlight all the materials mentioned in the protocol. Please click here to download this File.
Supplementary Figure 2: Ultrasound apparatus. This image showcases the buttons utilized for conducting a Doppler ultrasound examination. All the buttons described in the protocol are highlighted for easy reference. Please click here to download this File.
Supplementary Figure 3: Ultrasound apparatus in Pulse wave mode. The image demonstrates the buttons employed for conducting a Doppler ultrasound examination in Pulse wave mode. All the buttons mentioned in the protocol section are highlighted for clarity. Please click here to download this File.
Supplementary Figure 4: Doppler ultrasound signal. This image displays a blood velocity trace utilized for calculating leg blood flow. All the relevant metrics and buttons described in the protocol section are highlighted for easy identification and reference. Please click here to download this File.
