Quantitation of drug effects on puncture wound bleeding time
Puncture wound bleeding times provide a physiological model of a drug risk that can be readily carried out in mice. Outcomes that come from a puncture wound experiment are predictive. Here, we show a dabigatran dose-response bleeding curve. Dabigatran, a thrombin inhibitor, is used as an oral direct-acting anti-coagulant, a so-called DOAC12. The jugular vein puncture wound model was used to assess the risk inherent in different doses of dabigatran through potential prolonged bleeding through delayed thrombus formation in mice. A varying dosage of 15, 50, or 150 μg/kg of dabigatran was administered intravenously (i.v.) 20 min before the jugular vein puncture. We show the bleeding time means at various concentrations of dabigatran (Figure 4). At dose level, a significant prolongation of bleeding time is observed, p <0.051. This indicates a significant risk factor in the use of the drug in humans. Experimentally, the drug at these doses has a significant effect on the ultrastructure of the forming thrombus.
Assessing platelet activation state in a forming puncture wound thrombus
The WA-TEM approach provides both an overview of a wound area in a single plane when viewed at lower magnification and much detail at higher magnification (Figure 5). The details obtained can be directly placed within the context of the overview. We have used this approach to assess the recruitment of discoid-shaped platelets to a forming puncture wound thrombus. Circulating platelets are discoid, hence the name, and contain a full set of secretory granules. A key question has been how circulating platelets can be recruited to the growing thrombus without disturbing the free-flowing properties of the remaining platelets. Our work points to a Tether and Activate hypothesis in which circulating platelets are recruited to the thrombus, one by one, through a tethering process as discoid platelets containing a full set of organelles2. The evidence for this comes from WA-TEM of jugular vein thrombi 1 min post-puncture. Following sectioning to yield full thrombus slices from the middle of the still bleeding wound, we imaged 500-800 frames, 4,000 by 4,000 pixels, 3.185 nm pixel size in a rectangular XY raster grid across the complete dimension of the thrombus in cross-section using an automated stage and a transmission electron microscope using SerialEM software10. Frames were then stitched together using eTomo software, part of the IMOD program suite11. This results in a single image of varying size, for example, 120,000 pixels by 90,000 pixels that be full screen at low zoom, 0.02, or at detail at higher zoom, 0.25 to 1.0 using 3DMOD software, again a part of the IMOD program suite (Figure 5). In net, the software-driven analysis found that peripherally bound, thrombus-associated discoid platelets within the puncture hole were spaced apart as beads on a string. A short distance within the thrombus, the discoid shape was less distinct, and the platelets were more tightly associated with one another. Deeper within the thrombus, platelets were rounded, tightly packed, and partially degranulated. A sequence of morphology suggested the initial binding of platelets to the thrombus through a long tether molecule, likely von Willebrand factor, and that any further platelet activation steps were restricted to the interior of the forming thrombus. Hence, platelet recruitment to the thrombus could occur without disturbing the circulation of blood within the jugular vein.
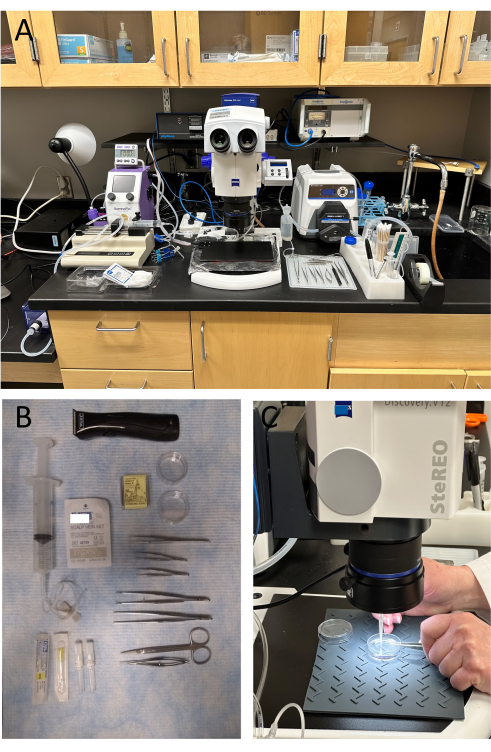
Figure 1: Surgical set-up to perform a jugular vein/femoral artery puncture wound thrombus experiment. Surgical equipment (A) and instruments (B) are carefully arranged for efficiency of movement since timing is critical during the experiment. (C) After perfusion fixation, the portion of the vessel containing the puncture wound thrombus is pinned to a silicone mat in a 35 mm culture dish while viewing under the light microscope. Please click here to view a larger version of this figure.
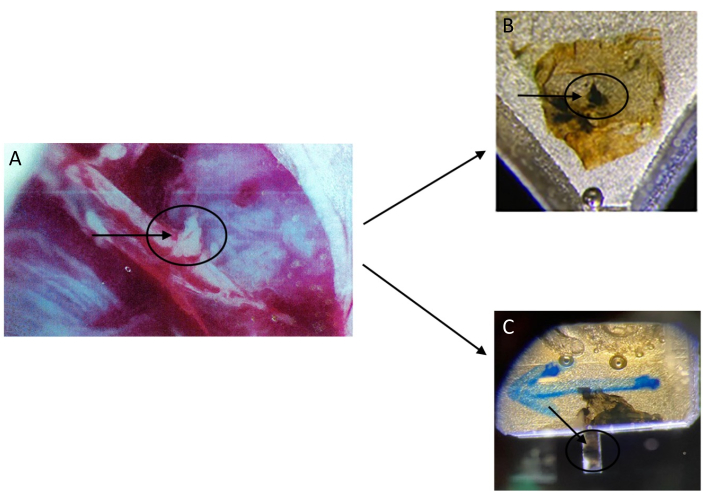
Figure 2: Going from a blood vessel to plastic embedded samples that will be sectioned for either WA-TEM or SBF-SEM. (A) A femoral artery with a puncture wound and accumulating extra-vascular thrombus formation (circle and arrow) is shown. (B) A thrombus (circle and arrow) is embedded in plastic for sectioning for WA-TEM with a microtome for subsequent 2D imaging. (C) A thrombus (circle and arrow) is embedded in plastic, trimmed to give a short stick, less than 1 mm, for attachment to a pin within an SBF-SEM imaging chamber. Please click here to view a larger version of this figure.
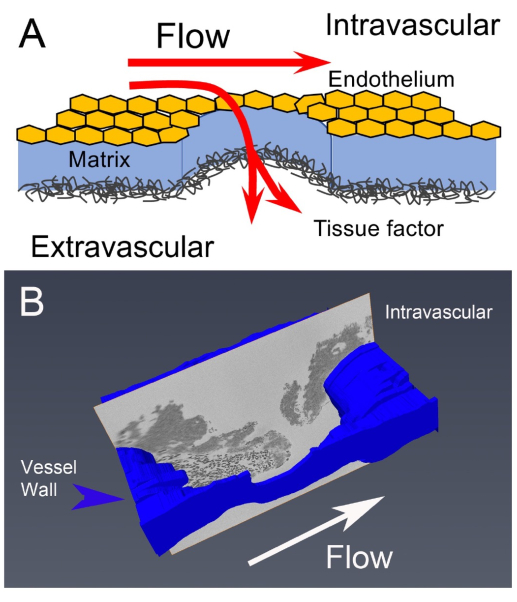
Figure 3: Puncture wound to thrombus formation: A schematic of preparative flow from a puncture wound (A) to an image slice of a 1 min post-puncture jugular vein thrombus (B). The vessel wall is labeled in blue on the image slice, the small black dots near the vessel wall are red blood cells, and the thrombus platelet aggregates appear as dark gray areas. This figure has been modified from1. Please click here to view a larger version of this figure.
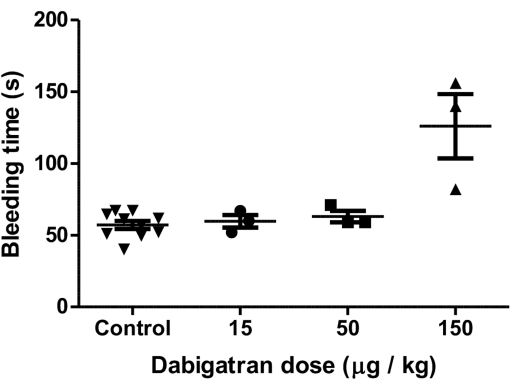
Figure 4: An example of data, in graphic form, generated in a jugular vein puncture wound experiment. A dabigatran dose-response bleeding curve is shown. This figure has been modified from1. The bleeding time means at various concentrations of dabigatran are shown along with error bars indicating plus or minus standard deviation. Statistical analysis using the student's t-test indicated a p-value of <0.05. Please click here to view a larger version of this figure.
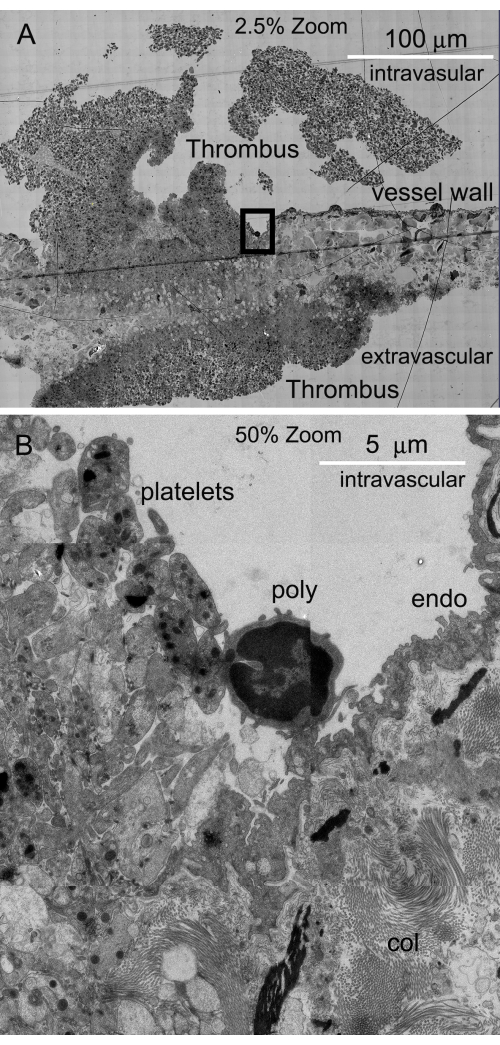
Figure 5: WA-TEM images of a slice stitched together to form a montage. (A) Individual high-resolution frames are collected and then stitched together for the purpose of placing features in a larger context. (B) By zooming up, important details can be brought out in context (poly: polymorphonuclear leukocyte, endo: endothelium, and col: collagen fibers). Please click here to view a larger version of this figure.
