The following protocol is for the production of a single microtube device.
1. Preparation of Halloysite Nanotube Solution
- Sonicate (10-13 W (rms)) 250 μL halloysite nanotube solution (6.6 wt% in water) 30 sec. Cool solution with cold water and repeat sonication once. Cool again.
- Draw sonicated solution into a syringe, attach a 0.45 μm syringe filter, and filter solution into clean microfuge tube. Vortex the solution occasionally to maintain homogeneity.
2. Coating of Microtube Inner Surface with Halloysite Nanotubes
- Obtain 50 cm long section of Micro-Renathane microtubing (300 μm inner diameter, 35.3 μL inner volume). Cut one end of the microtube at a diagonal and insert into a small IDEX adaptor piece. Insert the needle of a 3/10 cc 29G syringe into the other end of the microtube.
- To clean the microtube, place the open end of microtube (the end with the adaptor) into 70% ethanol and draw ~50 μL ethanol into the syringe to fill microtube.
- Rinse the ethanol out of the microtube by drawing a generous volume of distilled water into the syringe.
- Detach the syringe from the microtube, empty the syringe, and then reattach to the microtube.
- Prepare a solution of 0.02% w/v poly-L lysine in water. Draw 50 μL into the microtube and allow to sit for 5 min at room temperature (RT).
- Draw 100 μL filtered nanotube solution into the microtube and allow to incubate for 3 min at RT.
- Draw 100 μL water through the microtube to rinse out the nanotube solution. Allow coated microtube to sit, filled with water, overnight at RT.
3. Preparation of Microtubes for Cell Isolation
- Prepare a solution of 10 μg/mL protein G in 1X Dulbecco’s phosphate buffered saline (PBS, pH 7.0 – 7.2). Draw 50 μL PBS through microtube and then draw 50 μL of the protein-G solution and allow to incubate for 1.5 hr at RT.
- Prepare a solution containing 5 μg/mL E-selectin-IgG and 50 μg/mL antibody (anti-EpCAM for most cancer samples, anti-PSMA for prostate cancer samples) in PBS. Draw 50 μL of the E-selectin and antibody solution into the microtube and allow to incubate for 2 hr at RT.
- Nonspecific cellular adhesion is blocked with 5% milk protein. Prepare a solution of 5% (w/v) milk protein in PBS. Draw 50 μL milk protein solution into the microtube and allow to incubate for 1 hr at RT.
- Draw 50 μL PBS into tube and leave at RT until blood or buffy coat samples are ready for processing.
- 10 min prior to using the microtube for isolation, draw 50 μL PBS that has been saturated with Ca2+ (“PBS+”) to activate the selectin molecules.
4. Preparation of samples for cell isolation
- Draw or obtain 10 mL blood from patient into heparinized tube.
- Place 10 mL Ficoll-Paque lymphocyte isolation solution into 50 mL centrifuge tube. Gently layer 10 mL whole blood on top of Ficoll so as not to mix the blood and Ficoll.
- Centrifuge at 2000x g for 15 min at 4 °C with minimal deceleration.
- Remove the buffy coat layer and place in new tube.
- Wash buffy coat with PBS (centrifuge at 230x g for 10 min, discard the supernatant).
- Gently resuspend cells with 1 mL RBC lysis buffer and incubate for 10 min at RT to lyse erythrocytes.
- Add 10 mL PBS, mix gently, and centrifuge at 230x g for 10 min. Discard the supernatant and gently resuspend the pellet in 3 to 4 mL PBS+.
5. Cell isolation
- Attach one end of the functionalized microtube to a 5 mL syringe using IDEX adaptors.
- Insert the syringe onto a syringe pump.
- Submerge the open end of the functionalized microtube into the cell suspension.
- Process the cell suspension through the microtube at 1 to 4 mL/h.
- Transfer the open end of the microtube to a tube containing PBS+ and draw 300 μL PBS+ into syringe at 0.016 mL/min to remove unbound and loosely bound cells from the microtube.
- Place the open end of the microtube into a clean tube. Disconnect the syringe from the microtube and attach a syringe prefilled with Accutase. Gently perfuse enough Accutase into the microtube to fill (~50 μL) and allow to incubate at RT for 10 min.
- Attach a syringe prefilled with 1 mL of growth media (79% RPMI, 20% FBS, 1% penicillin streptomycin) and perfuse into microtube, collecting effluent into tissue culture treated well plate.
- Culture cells at 37 °C and 5% CO2 under humidified conditions.
6. Representative Results
The goal of this technique is to isolate viable cancer cells from the blood of cancer patients. Several methods exist to identify cancer cells in culture; a necessary verification of device success. We have chosen to stain cells in culture with antibodies against epithelial moieties such as EpCAM (epithelial cellular adhesion molecule) or PSMA (prostate specific membrane antigen), in addition to DAPI to identify intact cell nuclei (Fig. 2 and 3). The number of cancer cells captured using this technique is necessarily a function of the number of CTCs in the starting sample, and patient variability can be high. In processing samples taken from patients diagnosed with stage IV cancers, we routinely capture between 100 and 500 cancer cells per tube of blood, at purities >50%. Immediately following isolation, greater numbers of contaminating leukocytes may be present. However these numbers will be depleted following incubation in culture medium for up to 5 days.
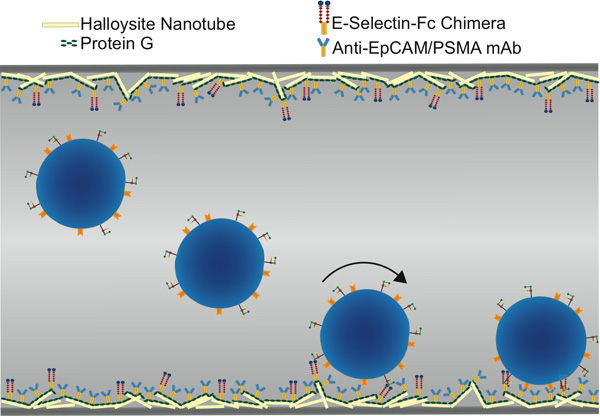
Figure 1. Schematic of functionalized microtube for CTC isolation, showing selectin-mediated rolling followed by antibody-mediated static adhesion.
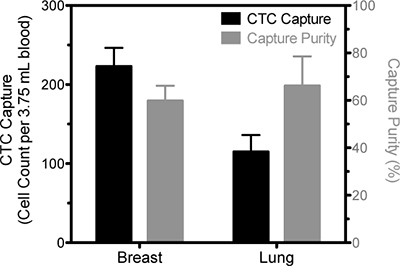
Figure 2. Representative data of CTC isolation from blood samples drawn from a breast cancer patient and a lung cancer patient. The number of viable cells positively identified as CTC based on EpCAM staining is represented by the solid bars and pertain to the left ordinate and the percentage of cells that were identified as CTC compared to the total number of captured cells is represented by the open bars and measured on the right ordinate. Results are following five days in culture.
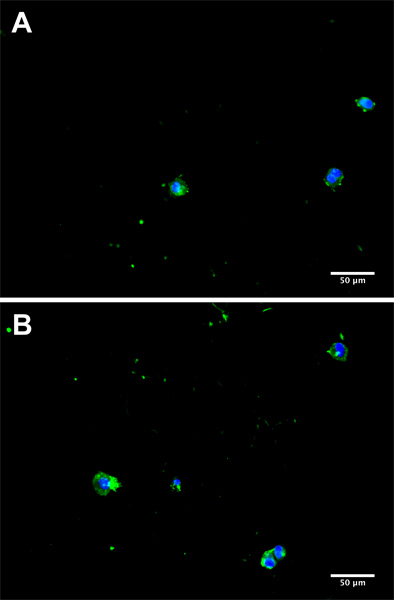
Figure 3. Representative micrographs from separate donors (A and B) of CTC in culture 5 days subsequent to isolation from a cancer patient blood sample. Cells were fluorescently stained for EpCAM with AlexaFluor 488 (green) and 4′,6-diamidino-2-phenylindole (DAPI) to visualize the nucleus (blue).
