We applied the described protocol to assess the biodistribution of a targeted probe, OsteoSense, which binds to hydroxyapatite. 3 mice (C57BL/6 Apoe-/- Ahsg-/- double knockout mice, 10 weeks old) were imaged before and 15 min, 2 h, 4 h, 6 h, and 24 h after i.v. injection of 2 nmol OsteoSense. Our software automatically detected the markers built into the multimodal mouse bed (Figure 1, Figure 2A,B), which enabled fusion of the anatomical µCT data with the fluorescence reconstruction performed by the FMT (Figure 2C,D). Since OsteoSense is a probe with a low molecular weight, a fast renal excretion and therefore high signal in the urinary bladder is expected. Fusion of the fluorescence reconstruction of the FMT revealed problems such as misplaced signal outside the bladder (Figure 2C,D). These problems occur because the FMT does not know the true shape of the mouse and assumes a block shape. Our reconstruction determines the accurate shape from the µCT data and generates scattering and absorption maps13 in order to enable a more accurate fluorescence reconstruction with better signal localization, which is particularly evident for the bladder (Figure 2E,F).
To assign the reconstructed fluorescence to appropriate regions, we interactively segmented several organs using our software (Figure 3). For each of the 18 scans, 7 regions were segmented based on the µCT data, i.e., heart, lung, liver, kidneys, spine, intestine and bladder. Subsequently, the software was used to compute the mean fluorescence concentration for each of the 126 regions. Fortunately, the software provides a batch mode, which computes all the values and saves them in a single spreadsheet.
To visualize the fluorescence distribution, 3D renderings were generated for each time point, using comparable windowing setting (Figure 4A-F). Using the quantified organ values, the biodistribution was computed by averaging the organ values over the three mice (Figure 4G). The pre scans, acquired before injection, showed negligible background signal. 15 min after injection, the strongest signal appeared in the urinary bladder, because of the fast renal excretion. At the subsequent time points, the remaining probe had accumulated at bones and joints.
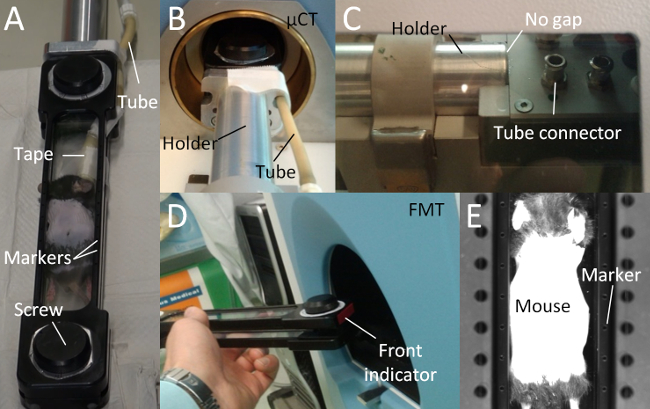
Figure 1. Multimodal Mouse Bed. (A) The multimodal mouse bed contains two acrylic glass plates that tightly hold the mouse. The tightening is adjusted using two screws. The mouse bed contains markers (empty holes) for image fusion. Anesthetic gas is supplied using a flexible tube which is fixated with tape. (B) The mouse bed is attached to a metal holder and held in the center of the rotating µCT gantry. (C) Avoid a gap between mouse bed and the metal holder, because otherwise, the markers may be incorrectly assigned leading to incorrect fusion. The anesthetic gas tube should be attached to the tube connector. (D) The mouse bed should be inserted into the FMT with the front first to enable a correct automated fusion. (E) The markers are visible to the FMT camera, which is used for the automated marker detection and fusion. Please click here to view a larger version of this figure.
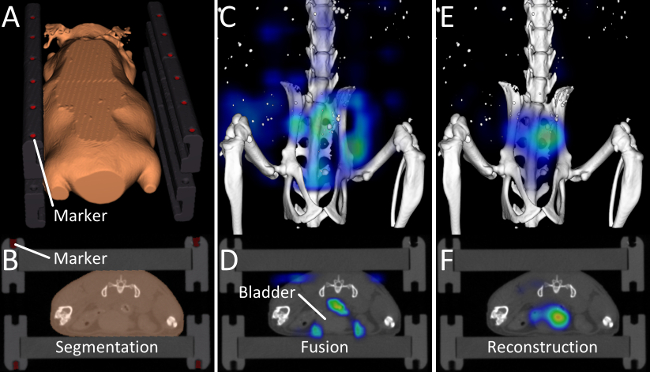
Figure 2. Image Fusion and Reconstruction. (A, B) Markers and the outer shape of the mouse are determined by the automated segmentation algorithm. (C, D) 15 min after injection of OsteoSense, a considerable amount of the probe has already been excreted into the urinary bladder. After fusing the vendor-provided reconstruction with the µCT data, problems become visible. Most of the signal appears around the bladder but not inside the bladder and some signal even appears in the air. This happens because the FMT assumes a block-shaped mouse. (E, F) Our improved fluorescence reconstruction, using the shape of the mouse derived from the µCT data, results in better localization of the fluorescence inside the bladder. Please click here to view a larger version of this figure.
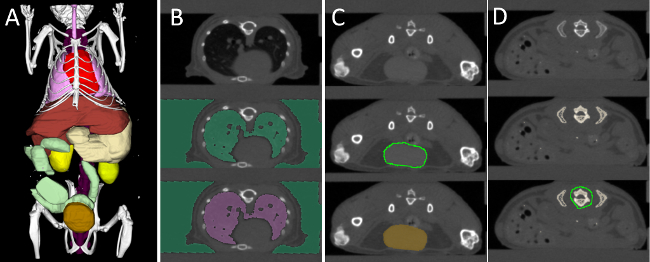
Figure 3. Interactive Organ Segmentation. (A) To quantify the fluorescence distribution, several organs are segmented: heart (red), lung (pink), liver (brown), stomach (beige), spine (purple), kidneys (yellow), intestine (green), and urinary bladder (gold). (B) The lung, which is strongly contrasted compared with the surrounding tissue, is segmented using thresholding and region filling. (C) Round organs, such as the bladder, kidneys, and heart are segmented using “scribbles”. (D) Organs with a more complex shape, e.g., liver and stomach are segmented incrementally using scribbles. To segment the spine, a high threshold is applied to segment all bones. Then some bones, e.g., the ribs, are cut away, until the spine remains. Please click here to view a larger version of this figure.
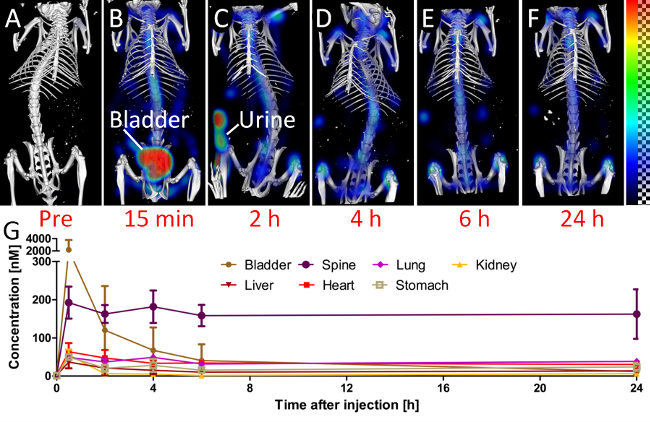
Figure 4. Biodistribution. To assess the biodistribution, the mice are scanned at several time points (A-F). (A) The pre scan, before injection, shows little background signal in the 750 nm channel. (B) 15 min after injection, a considerable amount of the probe is already in the urinary bladder. (C) At the 2 h time point, the mouse had urinated, which results in some fluorescence outside the mouse. At later time points (D-F), the signal appears predominantly at the bones and joints, i.e., at the spine and the knees. (G) The quantified fluorescence concentration is shown for selected organs.
