Note: A schematic overview of the study protocol is presented in Figure 1.

Figure 1. Study Protocol. This study protocol of normothermicex vivokidney perfusion is based on a porcine model. After surgical dissection of the vessels of the kidney graft and flushing with 500 ml of histidine-tryptophan-ketoglutarate (HTK), the graft can be retrieved. After cold storage (SCS) for 3 hrs, the kidney graft is perfused normothermic ex vivo (NEVKP) for multiple hours until the designated transplantation.
All animals received humane care in compliance with the ‘‘Principles of Laboratory Animal Care’’ formulated by the National Society for Medical Research and the ‘‘Guide for the Care of Laboratory Animals’’ published by the National Institutes of Health, Ontario, Canada. The Animal Care Committee of the Toronto General Research Institute approved all studies.
1. Animals
- Use male Yorkshire pigs (27 – 33 kg) in this protocol.
2. Organ Retrieval
- Preoperative Procedure
- House the male Yorkshire pigs in a research facility for at least one week to reduce their stress level. Fast the pigs for a minimum of 6 hrs before induction of the anesthesia.
- Initiate anesthetization of the pig by an intramuscular injection of ketamine (25 mg/kg), atropine (0.04 mg/kg), and midazolam (0.15 mg/kg). Subsequently, transport the animal from the housing facility to the operating room (OR).
- Place the pig in a supine position on the OR table. Let it breathe 2 L of oxygen with 5% of isoflurane spontaneously. After relaxation, expose the vocal cords with a laryngoscope and spray them with 2% lidocaine to prevent a spasm caused by intubation. After intubation with a 6.5 mm tube, block the cuff with 3 – 5 ml of air.
Note: Capnometry reveals the correct position of the tracheal tube. - Lower the isoflurane gas to 2.5%. Set the ventilator to 14 – 16 breaths/min and the tidal volume to 10 – 15 ml/kg bodyweight. Monitor the pig closely. Heart rate and oxygen saturation are recorded by pulse oxymetry.
- Under sterile conditions, introduce an 8.5 Fr. x 10 cm catheter into the jugular vein in Seldinger technique13. Therefore, use a needle to puncture the venous vessel. After introducing a wire, replace the needle with a catheter. Eliminate the wire and fix the catheter to the skin. Administer 200 ml of Ringer’s lactate solution per hour throughout the surgery.
- Surgical Procedure
- Following disinfection and coverage of the surgical field, perform a midline incision from xyphoid to pubic symphysis. To ameliorate the exposure, extend the surgical approach with a left lateral incision. Cover the large and small bowels with a towel and position them to the left side for optimal access to the right kidney.
- Separate the inferior vena cava (IVC) from the abdominal aorta. Ligate aortic branches from the back of the aorta.
- After complete aortic dissection to the back, pass a ligature around the aorta cranial to the renal branches. Additionally, place two ligatures cranial of the iliac bifurcation. Place a tie around the left renal artery.
- Free the right kidney from its adherent tissue. Dissect the renal vein, artery, and ureter.
- Open the diaphragm and administer 1,000 IU heparin per kg donor weight into the heart. For a DCD model, inject 40 mval of KCl intracardially 3 min after systemic heparinization to induce cardiac arrest. The cardiac arrest is valued as the starting point of warm ischemia.
- Meanwhile, for collection of blood, connect the lines of CPDA bags (citrate, phosphate, dextrose, adenosine) to the catheter introduced to the left upper jugular vein. Perform a soft spin (1,500 x g without brake). Remove plasma and buffy coat under sterile condition (biosafety cabinet class II) and store the erythrocytes for transfusion.
- Cannulate the aorta with an organ flush line above the iliac bifurcation. Tie the ligatures at the aorta and the left renal artery.
- Flush the kidney with histidine-tryptophan-ketoglutarate (HTK) solution with a pressure of 100 cm H2O. Clamp the thoracic cava and collect the blood via the jugular catheter. Cut the abdominal cava below the renal vein to secure an optimal flush of the kidney.
- After a complete flush of the right kidney, retrieve the graft with a segment of the aorta. Cut the renal vein and leave the ureter long.
- Back Table Preparation of the Kidney Graft for the Perfusion
- Free the kidney from adherent tissue. Close the cranial part of the aorta with a tie and cannulate the lower part with a 1/4” x 3/8” reducer. Tie off smaller arterial branches coming from the aorta.
- Cannulate the renal vein with a 1/4” x 3/8” reducer directly. Intubate the ureter with an 8 Fr. feeding tube.
- Place the kidney on ice until the start of the NEVKP.
3. Normothermic Ex vivo Kidney Perfusion (NEVKP)
- Preparation of the Perfusion Circuit
The perfusion circuit consists of neonatal cardiopulmonary bypass equipment (Figure 2).
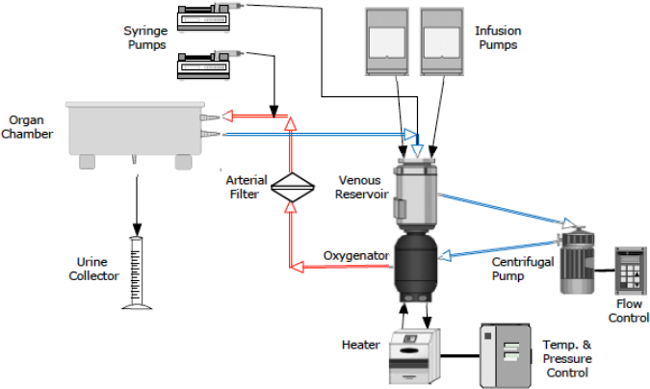
Figure 2. Schematic Drawing of the Perfusion Circuit. The circuit consists of neonatal cardiopulmonary bypass technology. The perfusion solution is collected in the venous reservoir. A centrifugal pump propels the solution into the oxygenator, where it is enriched with oxygen and warmed to 37 °C. After passing the arterial bubble filter, the perfusate is driven with a pressure of 60 – 80 mmHg through the renal artery into the kidney. The venous outflow (0 – 3 mmHg) leads the perfusate back into the venous reservoir. Syringe and infusion pumps secure the supply with additional compounds. The urine is collected throughout the perfusion. Perfusion circuit characteristics are recorded continuously. Hourly venous and arterial blood gas samples, and kidney injury markers are analyzed.- Connect the custom made perfusion circuit to the kidney perfusion device.
- Connect the tubing to the venous reservoir and oxygenator. Connect the arterial line tubing to the arterial outflow of the oxygenator and position the bubble filter in its holder. Connect the purge line. Connect the venous line tubing to the inlet of the venous reservoir.
- For assessment during the perfusion, plug the temperature probe into the arterial outlet, connect the flow meter and the bubble sensor to the arterial line tubing, and connect the pressure lines. Connect the level sensor.
- Connect the venous and arterial sample lines to the venous and arterial sample ports.
- Position the organ chamber on a stand and introduce the venous and arterial tubing through the prepared holes. Fix the tubing to the table and chamber firmly.
- Insert the suction tubing into the roller pump and position one end into the chamber to collect the fluids.
- Connect the oxygen tubing to the gas tank containing 95% O2 / 5% CO2 and the oxygenator. Connect the heating unit tubing to the oxygenator and the organ chamber.
- Use tubing clamps to close the venous and arterial outflow lines. Apply another tubing clamp to the outflow of the venous reservoir.
- Preparation of Perfusion Solution, Additional Supplements, and Priming the Circuit
- Use one infusion pump to replace the produced urine with Ringer’s lactate.
- Use one syringe pump to administer nutrition (glucose 0.5 ml/hr, amino acids 0.5 ml/hr) and insulin (5 IU/hr) into the venous reservoir. Utilize a second syringe pump to infuse a vasodilator (verapamil, 0.25 mg/hr) directly into the arterial line.
- Fill the venous reservoir with the perfusion solution. Therefore, pour Ringer’s Lactate (175 ml), STEEN solution (200 ml), dRO (27 ml), heparin (1,000 IU), sodium bicarbonate to adjust the pH, and calcium gluconate into the venous reservoir. Finally, add washed erythrocytes (125 ml).
- Switch on the heart lung machine (HLM). Activate the pressure, temperature, level, and bubble sensor panels. Activate the Data Management System (DMS) to record the data throughout the perfusion. Activate the heating unit to warm the perfusion solution and the organ chamber to 37 °C. Open the O2 supply.
- Open the tubing clamp behind the venous reservoir and free the centrifugal pump head from air completely. Start the centrifugal pump at 1,000 rpm and allow the solution to be propelled throughout the circuit. Clamp the tubing bypassing the arterial filter and release air from the arterial filter.
- Zero the pressure lines. Activate the syringe and infusion pumps.
- Kidney Graft Perfusion
- Remove the kidney from the ice, and position the kidney on bedding in the organ chamber. Place the urine catheter into the urine collector. After ensuring that the venous and the arterial tubing are free of air, plug the connectors to the tubing.
- Close the shortcut between the arterial and venous tubing lines. Set the arterial pressure to 75 mmHg by regulating the speed of the centrifugal pump.
- Record pressures, arterial flow, temperature, and presence of bubbles continuously with the DMS. Observe the values carefully throughout the perfusion. During the perfusion, blood leaking into the chamber is collected via the suction tubing back into the venous reservoir.
- Record the quantity of urine produced. Collect venous blood and urine samples hourly. Monitor the perfusion by taking venous and arterial blood gas samples and aspartate aminotransferase (AST), and lactate analysis.
- At the end of perfusion, disconnect the tubing from the renal artery and vein, flush the graft with cold HTK, and store it on ice in a sterile organ bag until transplantation.
In the following the results of six experiments using a model of heart-beating kidney retrieval are presented. After in situ flush and kidney retrieval, the grafts were stored on ice for 3 hr (SCS) while the erythrocytes were prepared. For the clinical setting, this simulates the time required for the retrieval and the back table preparation. NEVKP was performed for 10 hr.
To maintain physiological conditions and simulate an in vivo surrounding for the kidney, the organ chamber should be heated and sealed. Perfusion and urine replacement solution should represent physiological values for blood gas analysis, oncotic pressure, and osmolarity. Normal values (baseline values) obtained from Yorkshire pigs in situ, are located in each figure description, respectively (Figures 3 - 13). The aim of NEVKP is to ensure that the graft is supplied with sufficient oxygen and nutrition. As ischemia causes vasoconstriction, thus increasing intrarenal resistance, achieving a constant flow with a stable pressure is a good indicator for adequate oxygenation. After the target graft temperature of 37 °C is reached via rewarming of the organ after SCS, flow values and intrarenal resistance remain stable with a constant physiological pressure of around 60-80 mmHg throughout the whole perfusion (Figures 3 and 4). The quantity of urine production depends mainly on the composition of the perfusion solution (Figure 5).
Hourly measurements of venous and arterial pO2 reveal the metabolic activity of the kidney. The oxygen consumption was calculated using the equation ((pO2art – pO2ven) x flow / weight) (Figure 6) 14. During the perfusion pH, HCO3, and electrolytes are stable without requiring interventions (Figures 7 – 10). Real-time AST and lactate measurements serve to monitor cellular damage. No increase of parameters of cell injury is detected during the NEVKP period (Figures 11 and 12). The osmolarity of the perfusion solution is stable (Figure 13). Histological assessment reveals minor changes (Figure 14 – 16).
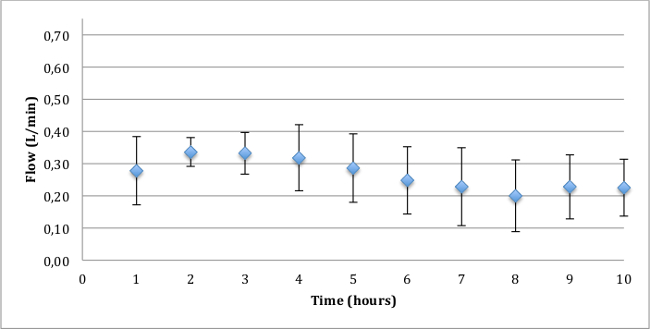
Figure 3. Mean arterial flow with standard deviation (ml/min). Throughout the perfusion the flow remains in a physiological range. Porcine physiological values, measured in situ: mean art. flow: 170 ± 57 ml/min (range 83 – 325 ml/min).
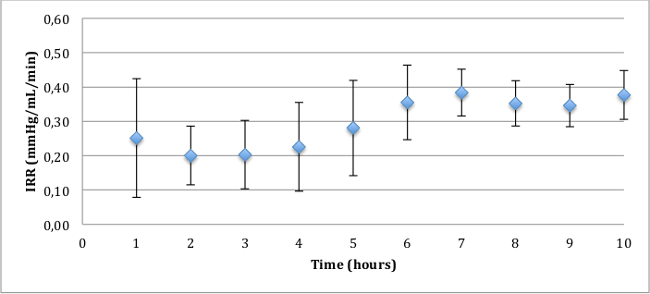
Figure 4. Intrarenal resistance (IRR), mean and standard deviation (mmHg/ml/min). The mean arterial pressure (MAP) remains constant between 60 and 80 mmHg. The intrarenal resistance is below 0.5 mmHg/ml/min constantly.
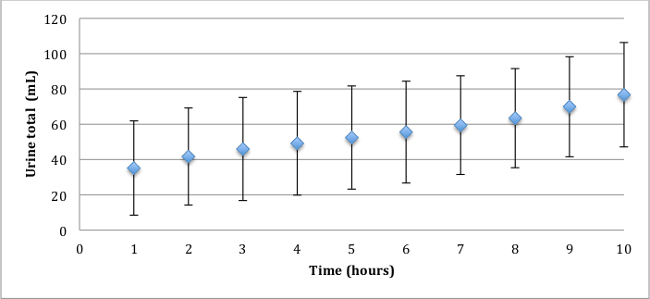
Figure 5. Total urine volume, mean and standard deviation (ml). The total urine volume mainly depends on the composition of the perfusion solution. The higher the oncotic pressure and the osmolarity, the lower the urine production.
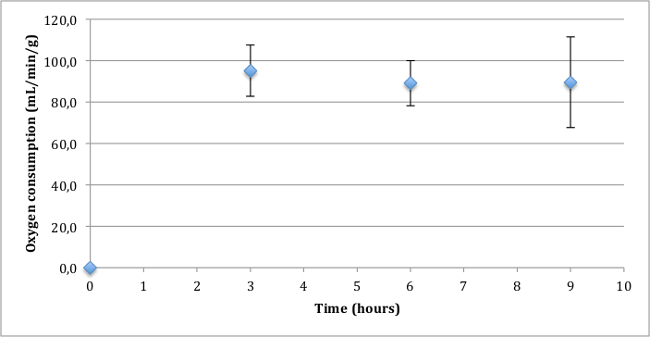
Figure 6. Oxygen consumption, mean and standard deviation (ml/min/g).
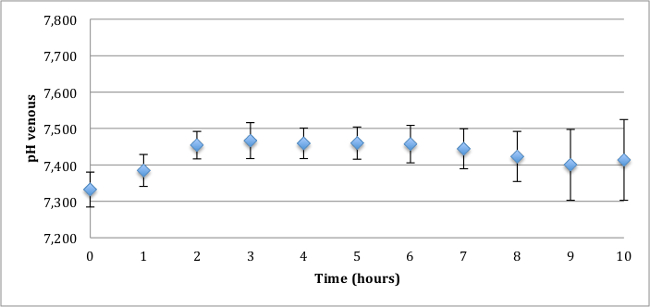
Figure 7. pH venous, mean and standard deviation. The pH remains constant in a physiological range without administration of bicarbonates. Porcine physiological values, measured in situ: pH 7.46 ± 0.06 (range 7.34 – 7.63).
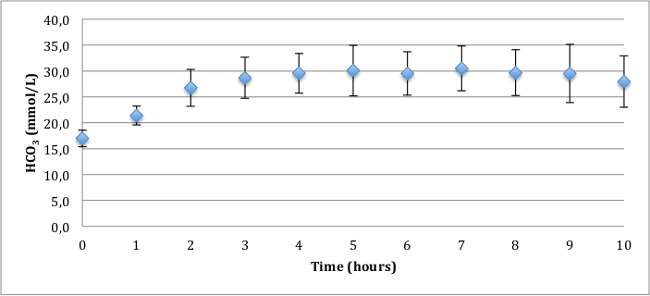
Figure 8. HCO3 venous, mean and standard deviation (mmol/l). The HCO3 remains in a physiological range without administration of bicarbonates. Porcine physiological values, measured in situ: HCO3 30.3 ± 2.4 mmol/L (range 21.6 – 35.8 mmol/L).
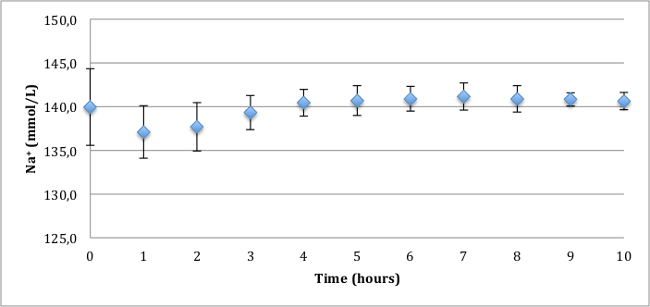
Figure 9. Venous sodium concentration, mean and standard deviation (mmol/L). The sodium remains in a physiological range. Porcine physiological values, measured in situ: 137.1 ± 3.8 mmol/L (range 118.7 – 140.9 mmol/L).
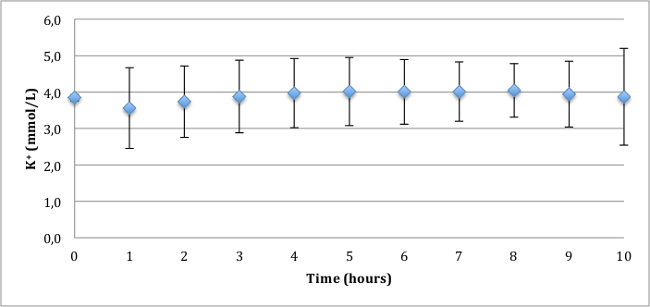
Figure 10. Venous potassium concentration, mean and standard deviation (mmol/L). The potassium remains constant in a physiological range. Porcine physiological values, measured in situ: 3.85 ± 0.46 mmol/L (range 3.5 – 5.36 mmol/L).
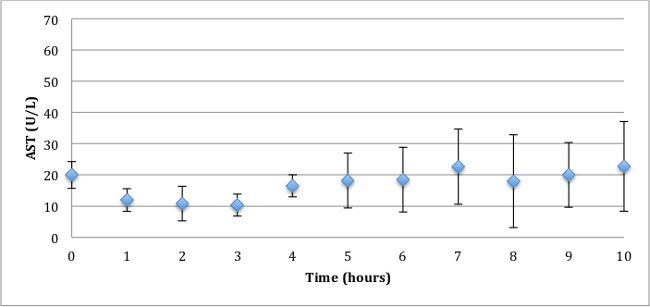
Figure 11. Venous aspartate aminotransferase, mean and standard deviation (AST; U/L). In the ex vivo normothermic kidney perfusion, AST demonstrates a cell injury marker. AST values are low throughout perfusion.
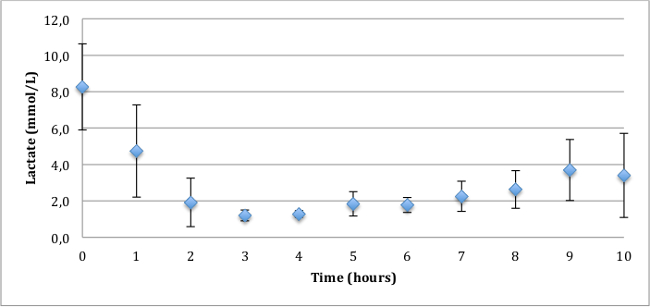
Figure 12: Lactate, mean and standard deviation (mmol/L). In the ex vivo normothermic kidney perfusion, lactate represents a cell injury marker. The values are stable throughout the perfusion.
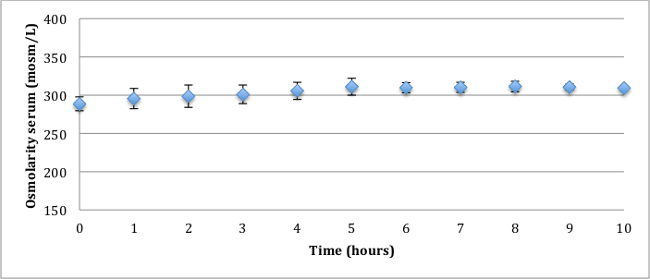
Figure 13: Osmolarity of the serum, mean and standard deviation (mosm/L). A constant osmolarity in the perfusion solution secures low but constant urine production. Porcine physiological values, measured in situ: 282 ± 1.7 mosm/L (range 279 – 283 mosm/L).
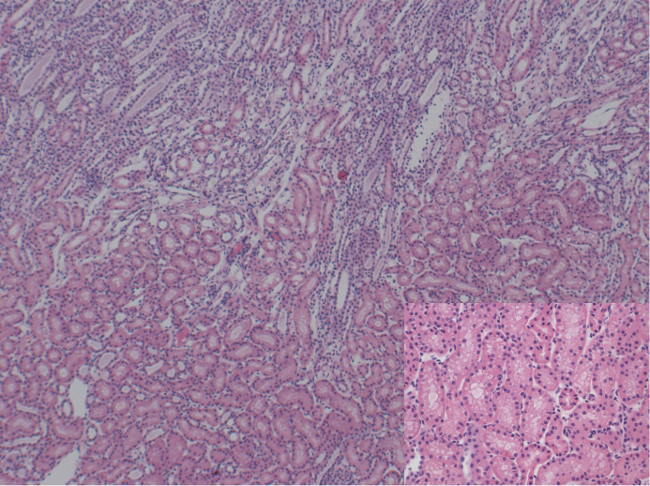
Figure 14: Histology (H&E). 50X / 200X magnification of corticomedullary junction showing mild tubular vacuolization. No signs of necrosis. Please click here to view a larger version of this figure.
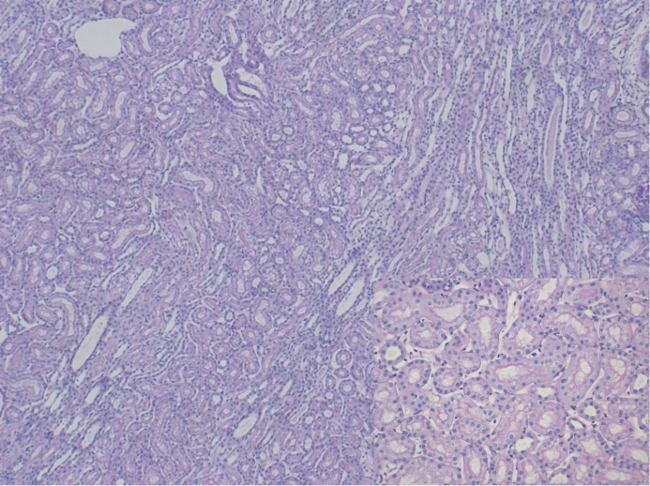
Figure 15: Histology (PAS). 50X / 200X magnification of corticomedullary junction showing mild tubular vacuolization. No signs of necrosis. Please click here to view a larger version of this figure.
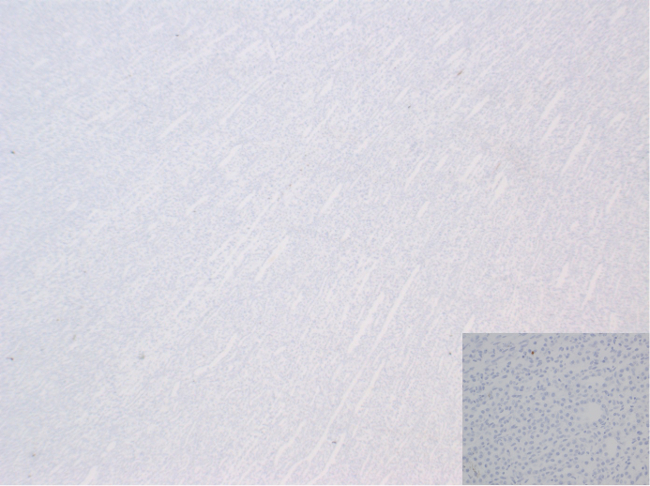
Figure 16: Histology (TUNEL staining). 25X / 200X magnification. Very occasionally nuclei are stained demonstrating very low rates of apoptosis. Please click here to view a larger version of this figure.
