A Protocol for the Administration of Real-Time fMRI Neurofeedback Training
Summary
The ability to induce and/or control neural plasticity may be critical in future treatments for neurologic disorders and the recovery from brain injury. In this paper, we present a protocol on the use of neurofeedback training with functional magnetic resonance imaging to modulate human brain function.
Abstract
Neurologic disorders are characterized by abnormal cellular-, molecular-, and circuit-level functions in the brain. New methods to induce and control neuroplastic processes and correct abnormal function, or even shift functions from damaged tissue to physiologically healthy brain regions, hold the potential to dramatically improve overall health. Of the current neuroplastic interventions in development, neurofeedback training (NFT) from functional Magnetic Resonance Imaging (fMRI) has the advantages of being completely non-invasive, non-pharmacologic, and spatially localized to target brain regions, as well as having no known side effects. Furthermore, NFT techniques, initially developed using fMRI, can often be translated to exercises that can be performed outside of the scanner without the aid of medical professionals or sophisticated medical equipment. In fMRI NFT, the fMRI signal is measured from specific regions of the brain, processed, and presented to the participant in real-time. Through training, self-directed mental processing techniques, that regulate this signal and its underlying neurophysiologic correlates, are developed. FMRI NFT has been used to train volitional control over a wide range of brain regions with implications for several different cognitive, behavioral, and motor systems. Additionally, fMRI NFT has shown promise in a broad range of applications such as the treatment of neurologic disorders and the augmentation of baseline human performance. In this article, we present an fMRI NFT protocol developed at our institution for modulation of both healthy and abnormal brain function, as well as examples of using the method to target both cognitive and auditory regions of the brain.
Introduction
Neurologic disorders present major impediments on affected individuals, their families, and society. Treatments for neurologic disorders can be non-existent or of questionable efficacy, and often only target symptoms of the disorder. Such is the case for tinnitus – the phantom perception of sound – which does not have a treatment approved by the U.S. Food and Drug Administration (FDA). Tinnitus can have a profound impact on a person's life, interfering with everyday tasks by decreasing concentration or altering the perception of actual sound. Furthermore, individuals affected by tinnitus may also experience fatigue, stress, sleep problems, memory problems, depression, anxiety, and irritability1. Therapies that do exist, such as antidepressant and antianxiety medications, only help manage the associated symptoms and may not treat the underlying cause. This creates a critical gap for innovative treatments of these disorders.
Improvements in acquisition techniques, computational power, and algorithms have revolutionized the speed with which functional Magnetic Resonance Imaging (fMRI) data can be measured and processed. This has enabled the advent of real-time fMRI, where data can be processed as it is collected. Early applications of real-time fMRI were limited2, primarily inhibited by the inability to rapidly complete the pre-processing steps typical to offline analyses such as motion correction. Improvements in computing technology and algorithms have now increased the speed, sensitivity, and versatility of real-time fMRI3 allowing similar offline pre-processing to be applied in real-time. These developments have led to 4 primary application domains of real-time fMRI: intraoperative surgical guidance4, brain-computer interfaces5,6, adapting stimuli for current brain states7, and neurofeedback training8.
NFT, although not the original focus of real-time fMRI, is a growing field of research where individuals learn to modulate brain activity volitionally through the implementation of mental strategies (i.e. imagined tasks). NFT is a form of operant conditioning9, which has been shown to increase neuronal firing rates and neuronal activity in monkeys10. Also, fMRI NFT has been associated with spike timing-dependent plasticity, which are neural changes that occur during associative learning11. Further implications suggest fMRI NFT induces plasticity via Long-Term Potentiation (LTP), resulting in enhanced synaptic efficiency12. Another postulation implies cellular mechanisms of skill learning, such as volitional control over brain activity, and may involve changes in voltage-dependent membrane conductance – expressed as a change in neural excitability13. In any case, it appears that fMRI NFT influences the brain at the neural level. These theories provide a strong case for the use of fMRI NFT in the treatment of neurologic disorders.
FMRI NFT, unlike traditional fMRI, offers the opportunity to investigate the relationship between brain activity and behavior11,14. Recently, there has been spike in studies involving fMRI NFT with almost twice as many articles published in 2011 – 2012 (n = 30) as compared to the previous 10 years (n = 16)11. One of the first fMRI NFT studies was conducted by Weiskopf and colleagues in 20038. This study successfully demonstrated the feasibility of online feedback and self-regulation of the fMRI signal in the Anterior Cingulate Cortex (ACC) using one participant. Feedback was displayed with a delay of approximately two seconds, more than an order of magnitude faster than the few previous studies. The first full study was conducted in 2004 where 6 participants learned to control activity of the somatomotor cortex15. FMRI NFT was completed across 3 sessions performed on the same day. Increased activity spatially selective to the target region in the somatomotor cortex was observed through the course of training at the single-subject and group levels. This effect was not observed for the control group which received real fMRI information from a background region (not correlated with the task being performed) earlier in the run. Researchers have since shown that humans can learn volitional control over the fMRI signal measured from numerous brain regions including the ACC16, amygdala17, anterior insula18,19, auditory and attention related networks20, bilateral rostrolateral prefrontal cortex21, dorsolateral prefrontal cortex12,22,23, motor cortices24,25,26,27,28, primary auditory cortex29,30, regions associated with emotional network regions31,32, right inferior frontal gyrus33, and visual cortices34,35.
The underlying mechanisms of many neurologic disorders are unknown. In the example of tinnitus, there is no obvious source for the phantom sound in the majority of cases36,37,38. Despite this, evidence suggests a central mechanism may be responsible for the tinnitus percept in some individuals, as demonstrated by the lack of symptom resolution after complete dissection of the auditory nerve39. Hyperactivity associated with tinnitus has been found in the primary auditory cortex40,41,42. Further evidence suggests that effects of tinnitus extend further into areas involved in the processing of emotion and attentional state43. Based on these abnormalities, fMRI NFT paradigms can be developed to induce and control neuroplastic mechanisms that encourage normal neural patterns.
Protocol
The following fMRI NFT protocol complies with the guidelines provided by the Wright State University Institutional Review Board.
1. Control Groups
- Carefully consider and determine control groups a priori. Design control group(s) to allow the hypothesis(es) to be evaluated and to account for effects from additional factors such as practice or expectations created by the feedback displays44.
2. Hardware Setup
- Prepare all hardware before the participant enters the MRI room using the same procedures as traditional fMRI.
- Connect the MR-compatible display and response device system to the stimulus computer (PC).
- Route cabling for the MR-compatible response devices and headphones through or around the MRI bore.
- Connect the TR-trigger output from the MRI to stimulus PC.
NOTE: In some setups, this may be connected to the MR-compatible response device hardware, which then connects to the stimulus computer. This is imperative for the synchronization stimuli and data acquisition. - Position the MR-compatible display so that it will be visible to the participant via the mirror (to be) affixed to the head coil.
3. Participant Positioning
NOTE: The participant should be positioned on the scanner table in a similar manner to a typical brain MRI, and in the same manner as traditional fMRI.
- Have the participant lie down in a supine position on the scanner table. Ask them to maintain their head inside the head coil.
- Place the headphones on the participant's head, and ensure the ears are covered. If additional hearing protection is required, insert ear plugs prior to positioning the head phones.
- Place a pad under the participant's knees for added comfort.
- Lock the upper body of the head coil into place.
- Affix the mirror to the head coil.
- Position the response devices in the participant's hands.
- Landmark the location of the participant's nasion relative to the scanner.
- Move the landmarked location to the center of the MRI bore.
- Confirm that the participant can view the entire display using the mirror. Ask the participant to adjust the mirror as necessary.
4. Localizing the Target Region
- Perform a "functional" localizer. Use the brain activity from the functional localizer to define the target Region of Interest (ROI)11.
NOTE: This run is executed in a similar manner to traditional fMRI. However, the target ROI can also be defined using individual anatomy or standardized atlases removing the need to perform a functional localizer.- Provide scripted and/or visual task instructions to the participant.
NOTE: These instructions should be concise but contain adequate information to allow the participant to successfully perform the task executed during the functional localizer.Here, the instructions inform the participant a dot will be on the screen and they may hear sounds in the headphones. Their goal is to relax and focus on the dot. - Begin synchronized administration of audible stimuli (e.g., bilateral continuous white noise29) and data acquisition by pushing the "Scan" button on the MR scanner.
NOTE: This is performed by programming the presentation of the stimuli using the TR trigger from the fMRI acquisition. The TR trigger is controlled via the fMRI protocol however this may be affected by the manufacturer of the MRI and the installed packages. Any visual, haptic, and/or auditory stimuli can be supplied to perform other tasks and/or target other regions.- Alternate the delivery of task stimuli (white noise) with matched control stimuli (no noise) in a blocked pattern. Use control stimuli to activate undesired networks/systems activated in the task stimuli.
NOTE: This alternation occurs by synchronizing stimuli to the fMRI acquisition and monitoring TR pulses. - Collect whole-brain echo planar images using a gradient-recalled-echo MRI pulse sequence; example parameters for the pulse sequence include an acquisition matrix of 64 x 64 elements in the phase and frequency directions, 41 slices aligned parallel to the anterior commissure-posterior commissure plane, 3.75 x 3.75 x 3 mm3 voxel size, 0.5 mm slice gap, fat suppression enabled, TR/TE = 2,000/20 ms, and a flip angle = 90°.
- Alternate the delivery of task stimuli (white noise) with matched control stimuli (no noise) in a blocked pattern. Use control stimuli to activate undesired networks/systems activated in the task stimuli.
- Provide scripted and/or visual task instructions to the participant.
- Compute an activation map from the fMRI data collected during the functional localizer using multivariate statistics.
NOTE: The following steps are a variant of processing performed for traditional fMRI. Some steps have been removed or simplified to decrease processing time.- Preprocess the data during data acquisition using custom software created from standard pre-processing techniques12,45.
- Perform 3D spatial filtering using a Gaussian low-pass kernel (full-width half-maximum of 4.5 mm).
- Correct for translational motion by aligning the center of mass for each volume to the first volume of the functional localizer using tri-linear interpolation.
- Perform temporal filtering using a Gaussian low-pass kernel with σ = 3 s.
- Create a model to predict the neurophysiological response to the task; this is performed in the same manner as traditional fMRI.
- Create a psychological model which describes the active and rest states for each time point46. This models the time points during the task with a value of '1' and control with a '0'.
- Convolve the psychological model with a predefined Hemodynamic Response Function (HRF)46 to predict the fMRI (neurophysiological) response to the task.
- Fit the fMRI data at each voxel as a function of time to the neurophysiological model using a General Linear Model (GLM). This results in a β parameter map, which is converted to t- or z-statistic maps (activation maps) using standard statistical transforms.
- Preprocess the data during data acquisition using custom software created from standard pre-processing techniques12,45.
- Use the activation map overlaid on a mean fMRI image to determine the region in which the feedback signal for the subsequent neurofeedback will be derived.
NOTE: This is performed using custom software. To remove global and unspecific changes, a second ROI may also be defined.- Navigate through the slices using the mouse slider wheel or the slice slider bar to find anatomical markers visible in the fMRI data such as the inferior surface of the frontal horn of the lateral ventricles12.
- Threshold the activation map using the threshold slider bar to reveal the voxels most robustly activated during the functional localizer in the target region.
- Perform this by selecting a threshold a priori or by manually adjusting the threshold.
- Use the left mouse button to select individual voxels with activation above the selected threshold and within the target region to add to the ROI.
NOTE: Voxels may be selected from one or more slices.
5. fMRI NFT
- Conduct neurofeedback runs using a boxcar model with alternating task and control conditions.
- Implement a task condition where participants raise or lower the activity of the target region, with the direction of control being critical to achieving the desired results.
NOTE: For example, many regions of the brain are hyperactive in patients with tinnitus and, therefore, decreasing activity may encourage normal neural patterns. - Alternate the task condition with a control condition where participants return activity to rest by relaxing and clearing their mind.
- Provide the participant with a scripted example of mindfulness tasks to be used during both conditions as starting aids for modulating brain activity towards the desired states. Instruct the participant to perform mindfulness tasks that drive brain activity towards the desired states.
- In the tinnitus example, instruct the participants to divert attention away from the auditory system to other sensory systems to reduce auditory activity.
- Baseline computation
NOTE: Due to tuning of the MRI hardware components prior to each run, baselines are used to normalize data prior to presenting feedback to the participant. The baseline average is determined for the target region using an average of one or more volumes acquired at the beginning of each fMRI NFT run12,47.- Instruct the participant to relax during a countdown presented at the beginning of the scan.
- Implement a task condition where participants raise or lower the activity of the target region, with the direction of control being critical to achieving the desired results.
- Begin synchronized stimuli presentation and data acquisition by pressing the "scan" button on the MRI scanner. Collect echo planar images using a gradient-recalled-echo MRI pulse sequence in the same manner as prescribed for the functional localizer in step 4.1.2.
- Acquire baseline volumes.
- Visually present a countdown timer and blank feedback display.
- Process the data during acquisition using custom software.
- Perform 3D spatial filtering using a Gaussian low-pass kernel (full-width half-maximum of 4.5 mm).
- Correct for translational motion using the center of mass for each volume; each volume is registered to the first volume of the functional localizer using tri-linear interpolation.
- Compute average signal from target ROI across both time and space.
- Sum the signals from all voxels within the target ROI in each volume.
- Create ROI average for each volume by dividing the sum by the number of voxels in the ROI.
- Average the sums from the baseline volumes.
- Acquire neurofeedback volumes
- Preprocess the data during acquisition using custom software.
- Perform 3D spatial filtering using a Gaussian low-pass kernel (full-width half-maximum of 4.5 mm).
- Correct for translational motion by aligning the center of mass for each volume to the first volume of the functional localizer using tri-linear interpolation.
- Compute the feedback signal. A feedback signal is derived from each acquired volume during fMRI NFT. This is the information that is presented to the participant to aid learning volitional control.
- Average the fMRI signal from all voxels within the target ROI to create a single value.
- Calculate the percent change between the current ROI average and the ROI baseline average. Optionally, this signal may be scaled by a factor dependent on the participant's performance.
- Compute the feedback signal by temporally filtering (Gaussian low-pass kernel with a sigma of 3 s consisting of only past components) the current percent change with the feedback signals from previous neurofeedback volumes.
- Display the feedback signal.
- Display the current feedback signal through a thermometer-style bar plot, where the height of the bar is proportional to the feedback value18,19,21,34.
- Overlay instructions for the participant on the feedback display.
NOTE: These instructions are simple, and should direct the participant to relax, or raise or lower activity (i.e. the thermometer bar).
- Optionally provide additional stimulation. Additional visual, auditory, or haptic stimulation may be presented concurrently with feedback.
- Preprocess the data during acquisition using custom software.
6. Assess the Ability to Self-regulate the Target ROI.
NOTE: After neurofeedback is completed, the ability to self-regulate the target region for each run of training needs to be quantified.
- Analyze intra-subject changes in the feedback signals12.
- Create a psychological model representing the rest and task conditions of neurofeedback.
NOTE: This model is convolved with a predefined HRF to produce a neurophysiological model. The process is the same as that described for the functional localizer. - Fit the feedback signal time series to the neurophysiological model using a GLM. This results in a β parameter, which is converted to t- or z-statistic representative of the ability to self-regulate.
- Create a psychological model representing the rest and task conditions of neurofeedback.
- Perform inter-subject comparisons.
NOTE: Statistics representative of self-regulation performance can be compared across runs and groups using appropriate statistical analyses (e.g., paired t-tests or ANOVAs). These tests evaluate changes in the ability to self-regulate the target region across training and groups, and can be used to evaluate the study's hypothesis(es).
Representative Results
Our team has demonstrated a significant increase in control over the left dorsolateral prefrontal cortex (DLPFC) learned from fMRI NFT in a cohort of 18 participants. A within-subjects one-way ANOVA was performed on the quantitative values of volitional control12. This analysis revealed control of the left DLPFC increased significantly across 5 x
6 min:24 s runs of neurofeedback separated across five separate sessions conducted within 14 d (Figure 1; F(4,68) = 2.216, p = 0.038, sphericity assumed, one-tailed). Changes in performance on a complex multitasking test, performed before and after NFT, were compared to a group which did not receive neurofeedback using 2 x 2 mixed-model ANOVAs. Post-hoc, Bonferroni-corrected comparisons revealed significant increases in performance on a complex multitasking test which did not receive additional training (p <0.005, one-tailed), and this increase was significantly greater than a control group which performed similar training but was not provided with the additional aid of neurofeedback (p <0.03, sphericity assumed, one-tailed)12. Despite the experiment group gaining control over the left DLPFC across training, a plateau was not observed. This signifies that maximum control is not necessary to produce behavioral results and that even greater effects may be possible with further training12. Furthermore, our team revealed fMRI NFT combined with n-back practice creates focal changes in brain activity that are confined to the target region and does not affect up- or down-stream components of the working memory network (Figure 2)22.
Regarding tinnitus, one previous study has investigated fMRI NFT as a possible treatment29. In this study, 4 x 4 min runs of neurofeedback were completed in a single training session. Behavioral assessments of tinnitus were conducted before and after the single fMRI NFT session. Successful volitional down-regulation of the auditory cortex was achieved, and led to a significant reduction in auditory activation. This study demonstrates the promise of fMRI NFT in treating tinnitus, however, only six participants were studied and a control group was not utilized for comparison. Furthermore, statistical analyses including the behavioral data were not performed. Expanding upon this study might reveal interesting new treatment opportunities for tinnitus patients.
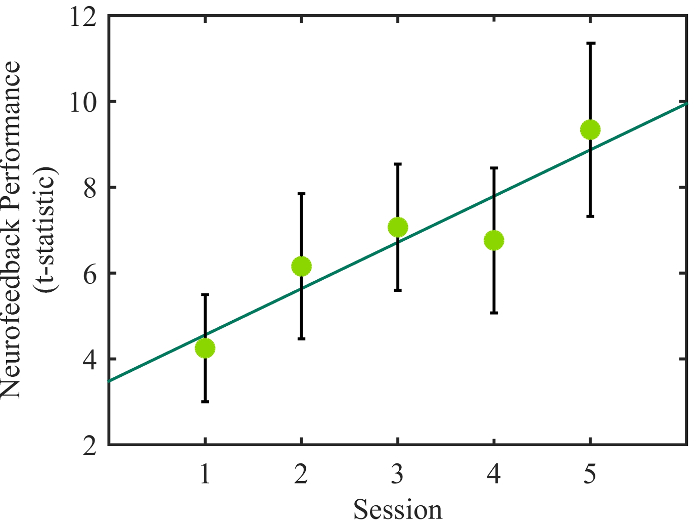
Figure 1: Increasing Control over Left DLPFC. Average left DLPFC control for each neurofeedback run (performed on separate days) are indicated by the light green circles. A linear regression analysis revealed a significant increase in control across training (dark green line; β = 1.078, p <0.033). Error bars represent 1 SEM. Unmodified work from Sherwood et al.12, reprinted under the Creative Commons Attribution license. Please click here to view a larger version of this figure.
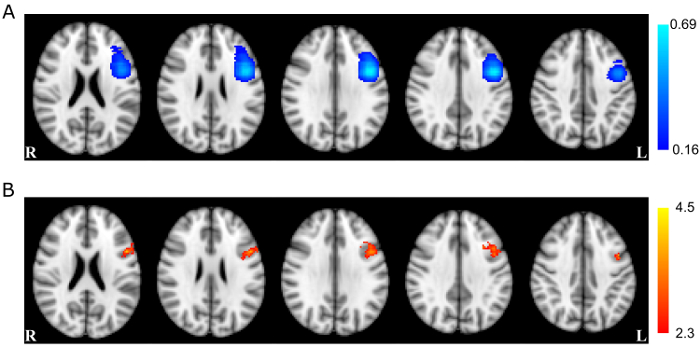
Figure 2: Localized Effect of Learning Left DLPFC Control. (A) The probability of voxel inclusion for fMRI NFT selected from an n-back functional localizer. Light blue voxels were included most frequently in the NFT target region, dark blue voxels were included less frequently, and clear voxels were not included. (B) Voxel-based ANOVA results for the main effect of training session (red-yellow). This effect showed a large overlap with the left DLPFC ROIs targeted for NFT. Axial slices are displayed in radiologic convention at the coordinates z = 22, 26, 30, 34, and 38 mm (left to right). Unmodified work from Sherwood et al.22, reprinted under the Creative Commons Attribution license. Please click here to view a larger version of this figure.
Discussion
The fMRI NFT protocol discussed herein can be adapted to target any region of the brain, and discusses a univariate, ROI-based approach to neurofeedback. This can be achieved by programming additional functional localizer tasks to activate other regions. By incorporating these tasks into the custom neurofeedback software, we have developed a very simple process. There is, however, one limitation: the target region must be functionally defined. At this time, the software that our team has developed does not perform any registration between functional and anatomical images. Therefore, other ROI selection methods, such as atlas-based ROIs, cannot be implemented at this time. In addition, parameters for the stimuli and neurofeedback (e.g., block duration, number of blocks, and imaging parameters including TR) can be easily manipulated by the operator. Additionally, transfer runs to evaluate the ability to self-regulate the target ROI in the absence of neurofeedback can be implemented. The software we have developed does not offer neurofeedback utilizing multivariate patterns35,48 or connectivity between brain regions49.
FMRI NFT offers significant advantages over other forms of neurofeedback but also has its limitations. The main advantage of fMRI NFT is the spatial resolution which outperforms all other forms of NFT such as electroencephalogram (EEG)-based neurofeedback. Enhanced spatial resolution enables specific brain structures/functions across the entire brain to be targeted50. Currently, this is not achievable with other therapies such as pharmacotherapy, which are systematic. However, the major drawback of fMRI NFT is the time delay. Not only are sampling rates much slower than EEG (up to 3 orders of magnitude slower), the hemodynamic lag associated with the fMRI signal further adds to this delay. Despite this, there is overwhelming evidence that participants can overcome this delay and, with practice, learn to control brain activity (e.g., for a review see Sulzer et al.11 and Scharnowski et al.50).
The popularity of fMRI NFT is growing but it remains in an infancy stage. Due to this, common practices have yet to be adopted. The described protocol details methods which are scientifically accepted. For example, multiple forms of feedback displays have been utilized across various studies, including a thermometer-style bar plot18,19,21,34. Furthermore, a feedback signal presented as the percent signal change with a baseline computed from the target region has also been extensively implemented12,19,21,25,30,51,52.
Controlling plastic effects in the brain offers an innovative therapeutic technique to treat neurologic disorders or brain injuries with abnormal brain activity, such as that associated with tinnitus discussed above. Although the exact mechanisms translating neuromodulation into behavioral effects are still unknown, fMRI NFT has been associated with LTP11. Through the learning process, behavior is reinforced when one actively regulates brain activity in task-related brain networks. Such reinforcement results in the engagement of neuroplastic mechanisms causing the network to execute more efficiently. This coincides with other NFT techniques such as EEG-based neurofeedback where individuals are trained to control frequency bands of electrical signals measured from local regions of the scalp53,54,55. Others have indicated LTP from synaptic plasticity resulting in enhanced synaptic efficiency12. Yet another postulation suggests cellular mechanisms of learning may involve changes in voltage-dependent membrane conductance which is expressed as a change in neural excitability13. In any case, it appears that fMRI NFT causes changes at the cellular level, and that the individual may learn some control over these processes. This ability and these changes may be critical in learning about and developing treatments for brain injuries and neurologic disorders.
An important aspect of fMRI NFT is to measure alterations in behavior. This is imperative to many hypotheses which predict behavioral changes driven by the NFT-induced neural changes. At a minimum, these assessments should be collected at two time points: prior to and following NFT. In the case of tinnitus, these behavioral assessments could consist solely of subjective questionnaires as there is no direct measure for tinnitus. For other neurologic disorders, a literature review should be conducted to determine the appropriate, reasonable, and documented assessments for the specific hypothesis(es) being investigated. Some hypotheses require measurements at additional time points, such as those exploring near-, short-, and long-term effects of fMRI NFT. Some assessments might require training prior to NFT to reduce learning effects. Other hypotheses might even require neurologic testing such as those interested in levels of brain metabolites, cerebral perfusion, or functional networks.
The fMRI NFT procedure has two critical stages. The first is determining a brain region to target for neurofeedback. Prior to conducting any procedures, a thorough literature review should be conducted to investigate neural pathways and important structures/functions associated with the neurologic disorder or brain injury. From this, key structures/functions should be carefully selected as the target for neurofeedback. Next, another literature review should be performed to examine tasks associated with this structure/function. This task may or may not be associated with the disorder, but it should be confirmed that the task activates the desired region(s) in the designated population. During neurofeedback procedures, this target region will be selected on an individual basis either at the first session or at each session. Therefore, inter- and intra-subject variability may be important factors which could lead to unpredictable results. It is critical to create a protocol to select the target region and conduct adequate personnel training. There are two methods to define a target ROI: anatomically and functionally. Anatomical definitions utilize structural MRI scans to define the target region strictly from anatomy, and possibly using a standard atlas. Functional images are registered to the structural images, and the target region is transformed into functional space21,26. In the functional method, the target region is selected from an activation map produced by conducting a functional localizer11,12,24,29,44. This method was discussed herein.
The second critical stage in fMRI NFT is control group selection. Control groups are crucial in determining the effect of fMRI NFT, and the selection of control groups should be carefully considered. Previous studies have used a wide range of controls. A common procedure for a control group is to attempt volitional control in the presence of sham feedback. This feedback can be yoked from a participant in the experimental group21,44, provided from a region not involved in the desired process unbeknownst to the participant17,33,44, or inverted52. Other studies have used control groups which attempt volitional control but are not provided with neurofeedback12,21,44,56.
A previous study suggests that when subjects attempt to control sham feedback, there is increased activation in the bilateral insula, anterior cingulate, supplementary motor, dorsomedial and lateral prefrontal areas when compared to passively watching a feedback display57. These findings implicate a broad fronto-parietal and cingulo-opercular network is activated when there is the intent to control brain activity. Furthermore, these findings suggest traditional control groups used in NFT experiments will use neural correlates consistent with cognitive control, even in the presence of sham feedback. A separate meta-analysis revealed activity in the anterior insula and basal ganglia, both of which are regions involved in cognitive control and other higher cognitive functions, were components critical to attempting volitional control58. The results of the meta-analysis corroborated the previous finding57. Taken together, this evidence suggests that it is critical to delineate effects of successful volitional control and those related to attempting self-regulation. Therefore, the inclusion of control groups which do not attempt self-regulation may be important.
However, previous studies where control groups received sham fMRI signals have revealed differences in target ROI activity were observed from those who received true feedback15,16,17,18,20,21,25,26,28,33,34,44, implying training strategies that do not incorporate feedback are not effective at modulating the target region. Additionally, control groups which received identical instructions and the same period of training but did not receive feedback on the current level of brain activity did not exhibit similar behavioral results as the experimental groups who were given neurofeedback12,18,21,32,44,59. These findings suggest the experiential effects are attributable to fMRI NFT-induced learning rather than other learning or nonspecific changes. Therefore, specific training regimens must be developed which target specific neurophysiological systems to obtain the desired effects. The results from a study with a variety of control groups indicate behavioral training, practice, sensory feedback, and biofeedback alone do not produce equivalent behavioral effects as those who receive fMRI NFT44.
Offenlegungen
The authors have nothing to disclose.
Acknowledgements
This material is based on research sponsored by the U.S. Air Force under agreement number FA8650-16-2-6702. The views expressed are those of the authors and do not reflect the official views or policy of the Department of Defense and its Components. The U.S. Government is authorized to reproduce and distribute reprints for Governmental purposes notwithstanding any copyright notation thereon. The voluntary, fully informed consent of the subjects used in this research was obtained as required by 32 CFR 219 and DODI 3216.02_AFI 40-402.
Materials
| 3T MRI | GE Medical | 750W Discovery | Data Acquisition Hardware |
| MR-Compatible Display System | InVivo | SensaVue | Visual Stimuli Hardware |
| MR-Compatible Auditory System | Resonance Technologies | CinemaVision | Auditory Stimuli Hardware |
| Experimental Stimulus Software | Neurobehavioral Systems | Presentation | Software to Control Stimuli Presentation |
| Experimental Processing Software | Mathworks | MATLAB | Software to Process Data |
| Data Processing Software | Microsoft | Visual Studio C++ | Software to Process Data |
| Response Pads | Cedrus Corporation | Lumina | Hardware to Receive Participant Input |
Referenzen
- Vanneste, S., Plazier, M., der Loo, E. V., de Heyning, P. V., Congedo, M., De Ridder, D. The neural correlates of tinnitus-related distress. NeuroImage. 52 (2), 470-480 (2010).
- Cox, R. W., Jesmanowicz, A., Hyde, J. S. Real-time functional magnetic resonance imaging. Magn Reson Med. 33 (2), 230-236 (1995).
- Weiskopf, N., et al. Real-time functional magnetic resonance imaging: methods and applications. P Int School Magn Reson Brain Funct. 25 (6), 989-1003 (2007).
- Hirsch, J., et al. An integrated functional magnetic resonance imaging procedure for preoperative mapping of cortical areas associated with tactile, motor, language, and visual functions. Neurosurgery. 47 (3), 711-722 (2000).
- Yoo, S. -. S., et al. Brain computer interface using fMRI: spatial navigation by thoughts. Neuroreport. 15 (10), 1591-1595 (2004).
- Sorger, B., Reithler, J., Dahmen, B., Goebel, R. A real-time fMRI-based spelling device immediately enabling robust motor-independent communication. Curr Biol. 22 (14), 1333-1338 (2012).
- Yoo, J. J., et al. When the brain is prepared to learn: Enhancing human learning using real-time fMRI. NeuroImage. 59 (1), 846-852 (2012).
- Weiskopf, N., et al. Physiological self-regulation of regional brain activity using real-time functional magnetic resonance imaging (fMRI): methodology and exemplary data. NeuroImage. 19 (3), 577-586 (2003).
- Fetz, E. E. Volitional control of neural activity: Implications for brain-computer interfaces. J Physiology. 579 (Pt 3), 571-579 (2007).
- Fetz, E. E. Operant Conditioning of Cortical Unit Activity. Science. 163 (3870), 955-958 (1969).
- Sulzer, J., et al. Real-time fMRI neurofeedback: Progress and challenges. NeuroImage. 76, 386-399 (2013).
- Sherwood, M. S., Kane, J. H., Weisend, M. P., Parker, J. G. Enhanced control of dorsolateral prefrontal cortex neurophysiology with real-time functional magnetic resonance imaging (rt-fMRI) neurofeedback training and working memory practice. NeuroImage. 124 (A), 214-223 (2016).
- Mozzachiodi, R., Byrne, J. H. More than synaptic plasticity: Role of nonsynaptic plasticity in learning and memory. Trends Neurosci. 33 (1), 17-26 (2010).
- Weiskopf, N., Scharnowski, F., Veit, R., Goebel, R., Birbaumer, N., Mathiak, K. Self-regulation of local brain activity using real-time functional magnetic resonance imaging (fMRI). J Physiology-Paris. 98 (4-6), 357-373 (2004).
- deCharms, R. C., Christoff, K., Glover, G. H., Pauly, J. M., Whitfield, S., Gabrieli, J. D. E. Learned regulation of spatially localized brain activation using real-time fMRI. NeuroImage. 21 (1), 436-443 (2004).
- Hamilton, J. P., Glover, G. H., Hsu, J. -. J., Johnson, R. F., Gotlib, I. H. Modulation of subgenual anterior cingulate cortex activity with real-time neurofeedback. Hum Brain Mapp. 32 (1), 22-31 (2011).
- Zotev, V., et al. Self-regulation of amygdala activation using real-time fMRI neurofeedback. PLoS ONE. 6 (9), e24522 (2011).
- Caria, A., et al. Regulation of anterior insular cortex activity using real-time fMRI. NeuroImage. 35 (3), 1238-1246 (2007).
- Veit, R., Singh, V., Sitaram, R., Caria, A., Rauss, K., Birbaumer, N. Using real-time fMRI to learn voluntary regulation of the anterior insula in the presence of threat-related stimuli. Soc Cogn Affect Neur. 7 (6), 623-634 (2012).
- Lee, J. -. H., Kim, J., Yoo, S. -. S. Real-time fMRI-based neurofeedback reinforces causality of attention networks. Neurosci Res. 72 (4), 347-354 (2012).
- McCaig, R. G., Dixon, M., Keramatian, K., Liu, I., Christoff, K. Improved modulation of rostrolateral prefrontal cortex using real-time fMRI training and meta-cognitive awareness. NeuroImage. 55 (3), 1298-1305 (2011).
- Sherwood, M. S., Weisend, M. P., Kane, J. H., Parker, J. G. Combining real-time fMRI neurofeedback training of the DLPFC with n-back practice results in neuroplastic effects confined to the neurofeedback target region. Front Behav Neurosci. 10 (138), 1-9 (2016).
- Zhang, G., Yao, L., Zhang, H., Long, Z., Zhao, X. Improved working memory performance through self-regulation of dorsal lateral prefrontal cortex activation using real-time fMRI. PLoS ONE. 8 (8), e73735 (2013).
- Sitaram, R., et al. Acquired control of ventral premotor cortex activity by feedback training: an exploratory real-time fMRI and TMS study. Neurorehab Neural Re. 26 (3), 256-265 (2012).
- Subramanian, L., et al. Real-time functional magnetic resonance imaging neurofeedback for treatment of Parkinson’s Disease. J Neurosci. 31 (45), 16309-16317 (2011).
- Yoo, S. -. S., Lee, J. -. H., O’Leary, H., Panych, L. P., Jolesz, F. A. Neurofeedback fMRI-mediated learning and consolidation of regional brain activation during motor imagery. Int J Imag Syst Tech. 18 (1), 69-78 (2008).
- Berman, B. D., Horovitz, S. G., Venkataraman, G., Hallett, M. Self-modulation of primary motor cortex activity with motor and motor imagery tasks using real-time fMRI-based neurofeedback. NeuroImage. 59 (2), 917-925 (2012).
- Chiew, M., LaConte, S. M., Graham, S. J. Investigation of fMRI neurofeedback of differential primary motor cortex activity using kinesthetic motor imagery. NeuroImage. 61 (1), 21-31 (2012).
- Haller, S., Birbaumer, N., Veit, R. Real-time fMRI feedback training may improve chronic tinnitus. Eur Radiol. 20 (3), 696-703 (2010).
- Haller, S., et al. Dynamic reconfiguration of human brain functional networks through neurofeedback. NeuroImage. 81, 243-252 (2013).
- Johnston, S. J., Boehm, S. G., Healy, D., Goebel, R., Linden, D. E. J. Neurofeedback: A promising tool for the self-regulation of emotion networks. NeuroImage. 49 (1), 1066-1072 (2010).
- Johnston, S., Linden, D. E. J., Healy, D., Goebel, R., Habes, I., Boehm, S. G. Upregulation of emotion areas through neurofeedback with a focus on positive mood. Cogn Affect Behav Ne. 11 (1), 44-51 (2011).
- Rota, G., et al. Self-regulation of regional cortical activity using real-time fMRI: The right inferior frontal gyrus and linguistic processing. Hum Brain Mapp. 30 (5), 1605-1614 (2009).
- Scharnowski, F., Hutton, C., Josephs, O., Weiskopf, N., Rees, G. Improving visual perception through neurofeedback. J Neurosci. 32 (49), 17830-17841 (2012).
- Shibata, K., Watanabe, T., Sasaki, Y., Kawato, M. Perceptual learning incepted by decoded fMRI neurofeedback without stimulus presentation. Science. 334 (6061), 1413-1415 (2011).
- Fowler, E. Head noises in normal and in disordered ears: Significance, measurement, differentiation and treatment. Arch Otolaryngol. 39 (6), 498-503 (1944).
- Penner, M. J. An estimate of the prevalence of tinnitus caused by spontaneous otoacoustic emissions. Arch Otolaryngol. 116 (4), 418-423 (1990).
- Sismanis, A., Smoker, W. R. K. Pulsatile tinnitus: Recent advances in diagnosis. Laryngoscope. 104 (6), 681-688 (1994).
- Folmer, R. L., Griest, S. E., Martin, W. H. Chronic tinnitus as phantom auditory pain. Otolaryngology. 124 (4), 394-400 (2001).
- Gu, J. W., Halpin, C. F., Nam, E. -. C., Levine, R. A., Melcher, J. R. Tinnitus, diminished sound-level tolerance, and elevated auditory activity in humans with clinically normal hearing sensitivity. J Neurophysiol. 104 (6), 3361-3370 (2010).
- Schecklmann, M., et al. Neural correlates of tinnitus duration and distress: A positron emission tomography study. Hum Brain Mapp. 34 (1), 233-240 (2013).
- Geven, L. I., de Kleine, E., Willemsen, A. T. M., van Dijk, P. Asymmetry in primary auditory cortex activity in tinnitus patients and controls. Neurosci. 256, 117-125 (2014).
- Seydell-Greenwald, A., Leaver, A. M., Turesky, T. K., Morgan, S., Kim, H. J., Rauschecker, J. P. Functional MRI evidence for a role of ventral prefrontal cortex in tinnitus. Brain Res. 1485, 22-39 (2012).
- deCharms, R. C., et al. Control over brain activation and pain learned by using real-time functional MRI. P Natl Acad Sci USA. 102 (51), 18626-18631 (2005).
- Friston, K. J., et al. Analysis of fMRI time-series revisited. NeuroImage. 2 (1), 45-53 (1995).
- Ashby, F. G. . Statistical analysis of fMRI data. , (2011).
- Ruiz, S., et al. Acquired self-control of insula cortex modulates emotion recognition and brain network connectivity in schizophrenia. Hum Brain Mapp. 34 (1), 200-212 (2013).
- Papageorgiou, T. D., Curtis, W. A., McHenry, M., LaConte, S. M. Neurofeedback of two motor functions using supervised learning-based real-time functional magnetic resonance imaging. Eng Med Biol Soc Ann. , 5377-5380 (2009).
- Koush, Y., et al. Connectivity-based neurofeedback: Dynamic causal modeling for real-time fMRI. NeuroImage. 81, 422-430 (2013).
- Scharnowski, F., Weiskopf, N. Cognitive enhancement through real-time fMRI neurofeedback. Curr Opin Behav Sci. 4, 122-127 (2015).
- Sulzer, J., et al. Neurofeedback-mediated self-regulation of the dopaminergic midbrain. NeuroImage. 83, 817-825 (2013).
- Berman, B. D., Horovitz, S. G., Hallett, M. Modulation of functionally localized right insular cortex activity using real-time fMRI-based neurofeedback. Front Human Neurosci. 7 (638), 1-11 (2013).
- Birbaumer, N., Cohen, L. G. Brain-computer interfaces: Communication and restoration of movement in paralysis. J Physiol. 579 (3), 621-636 (2007).
- Daly, J. J., Wolpaw, J. R. Brain-computer interfaces in neurological rehabilitation. Lancet Neurol. 7 (11), 1032-1043 (2008).
- Ros, T., Munneke, M. A. M., Ruge, D., Gruzelier, J. H., Rothwell, J. C. Endogenous control of waking brain rhythms induces neuroplasticity in humans. Eur J Neurosci. 31 (4), 770-778 (2010).
- Linden, D. E. J., et al. Real-Time Self-regulation of emotion networks in patients with depression. PLoS ONE. 7 (6), e38115 (2012).
- Ninaus, M., et al. Neural substrates of cognitive control under the belief of getting neurofeedback training. Front Hum Neurosci. 7 (914), 1-10 (2013).
- Emmert, K., et al. Meta-analysis of real-time fMRI neurofeedback studies using individual participant data: How is brain regulation mediated?. NeuroImage. 124, 806-812 (2016).
- Linden, D. E. J., Turner, D. L. Real-time functional magnetic resonance imaging neurofeedback in motor neurorehabilitation. Curr Opin Neurol. 29 (4), 412-418 (2016).
