When proper skin preparation is conducted, perceptual thresholds are inversely correlated with stimulation pulse width. As pulse width increases, the perceptual threshold decreases (Figure 7). Initial studies by this group exploring the effect of pulse width on PT in healthy individuals (meeting inclusion/exclusion criteria listed above), determined that the combined overall (n=15, 7 female, mean age 26.5 ± 4.99) PT at 100 μs = 3.92 ± 1.1 mA; 200 μs = 2.24 ± 0.74 mA; 500 μs = 1.24 ± 0.41 mA. These thresholds suggest that a constant current stimulator with capacity of delivering up to 5 mA of current is required for stimulation of 500 μs pulse width parameters, and a minimum of a 10mA stimulator is required for lower pulse widths (Table 2). Fine tuning of the current is required, with increments of 0.1 mA are necessary for precise stimulation.
Delivering stimulation at 200% PT is tolerable and relatively pain free as demonstrated by pain numerical rating scales (NRS) scales9,30. The NRS scale is a rating system for pain from 0-10 in which individuals report pain or discomfort29. Both Active and Sham stimulation rate similarly low pain levels (NRS <3 for all stimulation pulse widths. More specifically, the biologically-active pulse width of 500 μs delivered at 25 Hz is reported on average to rate as Active = 1.98 ± 0.83, Sham = 2.17 ± 1.27 (n=25, 9 female, mean age 25.16 ± 4.16 years) (Table 3). Pain ratings for other parameters are no more painful than the 25 Hz parameter and the details can be found in the groups' prior work30.
Safety and tolerability of 30 min to 1 hour sessions at a 20–50% duty cycle has been widely reported in the literature with some studies delivering multiple sessions in the same day spread 12–15 h apart12,31. No serious adverse events have been reported from 60 subjects participating in several series of experiments with subjects participating from 1 to 8 repeated visits spread a minimum of 24 hours apart.
taVNS, when administered as reported in this manuscript, has been demonstrated to modulate the autonomic nervous system, induce functional brain activity changes as measured by fMRI BOLD, and piloted to treat neuropsychiatric disorders and aid in rehabilitation.
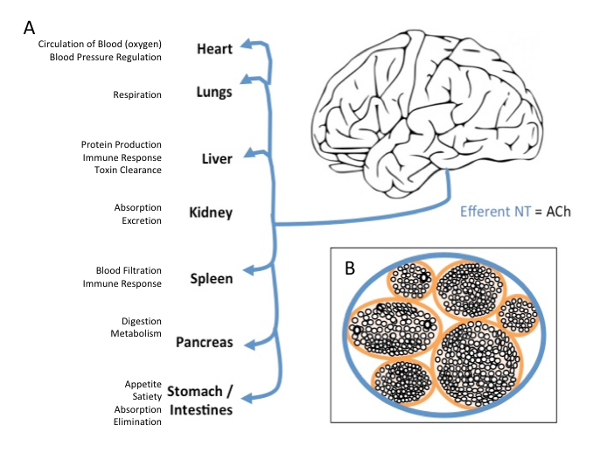
Figure 1: Vagus Nerve Efferent Projections and Cross-section. (A) Efferent projections of the vagus nerve target every major organ on the body with wide effects on bodily function (B) Cross-section of the vagus nerve, demonstrating the inside anatomy of the nerve as a series of bundles of nerves all contained within one major pathway. Please click here to view a larger version of this figure.
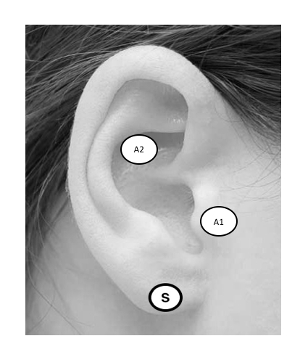
Figure 2: taVNS Ear Targets. Targeting the ABVN can be accomplished by stimulating the anterior wall of the outer ear canal, landmarked notably by the tragus (A1), or cymba conchae (A2). Sham stimulation is administered to the earlobe (S). Please click here to view a larger version of this figure.
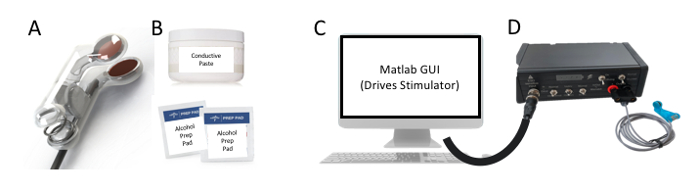
Figure 3: Key Components. The minimum required components for proper administration of taVNS are the following (A) ear stimulation electrodes, (B) conductive gel and alcohol prep pads, (C) computer capable of sending and receiving TTL pulses to a (D) constant current stimulator to trigger stimulation. Please click here to view a larger version of this figure.
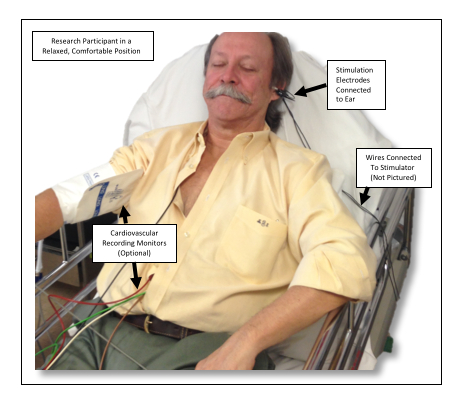
Figure 4: Example Setup. This photo shows an individual receiving taVNS of the left ear while in position to undergo an experimental paradigm. Please click here to view a larger version of this figure.
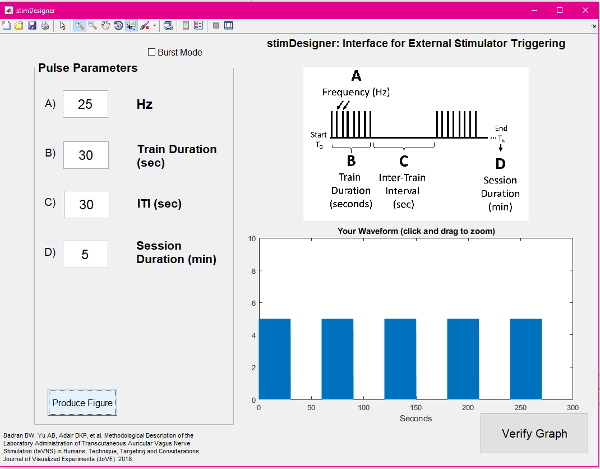
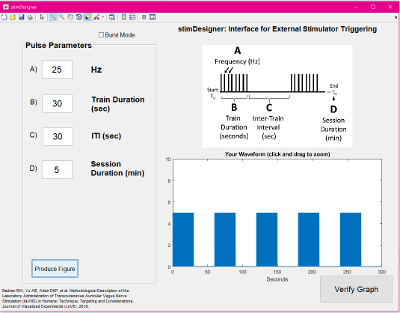
Figure 5: Screenshot of the GUI used for stimulation. Please click here to view a larger version of this figure.
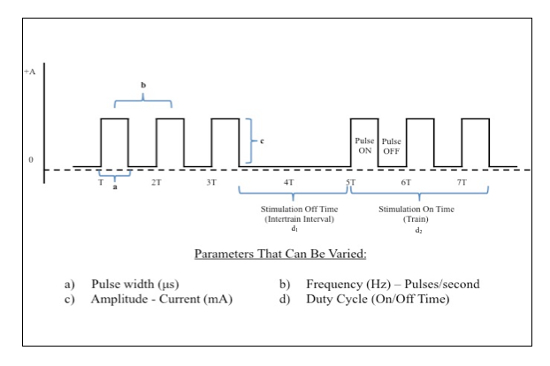
Figure 6: Electrical Stimulation Waveform Manipulations. Direct square wave electrical current can be delivered at various parameters. This figure demonstrates key properties of the waveform that can be changed in order to achieve desired biologic effects. Please click here to view a larger version of this figure.
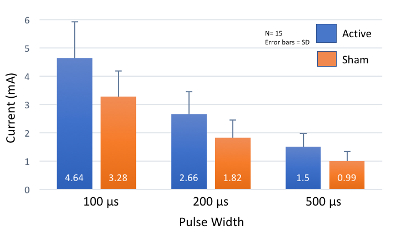
Figure 7: Perceptual Threshold Values at Increasing Pulse Widths. As pulse width increases, perceptual threshold (PT) decreases. Most healthy individuals will have a PT within 2 standard deviations (SD) of these mean values. Please click here to view a larger version of this figure.

Table 1: Example of How to Determine Perceptual Threshold (PT). This table shows an example sequence of Yes/No responses used to parametrically determine PT.
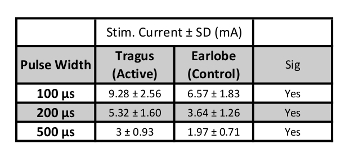
Table 2: Stimulation Current Levels. Values of stimulation current in mA (200% PT) for each pulse width (n=15).

Table 3: PT, Stimulation Current, and Pain Values for Suggested Stimulation Parameters. Values of stimulation current in mA (200% PT) for each pulse width (n=25).
Supplemental File: Freeware GUI used in this protocol. Please click here to download this file.
