Experience in using this approach in 43 patients with severe TBI was recently published17. Patient selection limits the number of those eligible, but focusing on only those with TBI at a level I trauma center led to approximately 2 patients per month. This number is predicated on hospital volume and may increase if additional acute brain injuries are considered for monitoring, such as those with hemorrhagic stroke.
Placement may take place either in patients with non-surgical severe injuries or in those who have undergone surgery, depending on the preferences at an individual institution (Figure 1). This technique has been performed within a median of 12.5 h (interquartile range [IQR] 9.0–21.4 h) of injury and probes have been left in situ for a median of 97.1 h (IQR 46.9–124.6 h)17. Placement is typically within the non-dominant frontal lobe unless there is a contraindication. Three-quarters of bolts placed in dominant frontal lobe were placed contralateral to prior craniectomy. Nonetheless, in TBI, this strategy led to placement within an injured lobe the majority of the time. Misplacement was rare using this technique, occurring in only 6/42 (14.3%) of patients; device measurements were rarely affected17.
Bedside placement resulted in no adverse events at the time of bolt insertion. On follow up CT, small regions of peri-probe hematoma, pneumocephalus, or bone chips were found in 40.5% of patients17. However, mirroring the experience of other institutions18 that perform similar monitoring, only one expanding hematoma was considered to be a major hemorrhage. In this case, no surgical or medical intervention was recommended, and the patient outcome was felt not to be impacted. Across two cohorts including patients with TBI and subarachnoid hemorrhage, the overall rate of significant hemorrhage is 1.9%17,18.
Once devices are in place, device dislodgement may occur and has been described as being related to the size of the probes, length of time they remain in situ, and relative complexity of moving, transferring, and caring for this patient population. More than half of patients experienced dislodgement of at least one probe before the end of their recording period, mostly commonly the rCBF probe. Limiting transportation may mitigate this risk: the number of trips that patients took appeared to be associated with devices becoming dislodged or no longer functioning (Wilcoxon rank sum test, p = 0.03)17. Nonetheless, this technique has resulted in measurements of all modalities in more than 90% of placements and most probes remain in place and generate continuous data for >90% of the recording period.
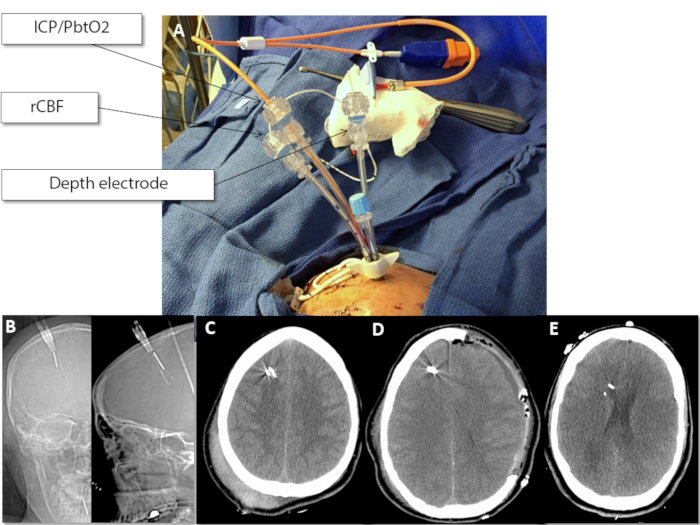
Figure 1: Clinical and radiologic placement of multimodality monitoring probes. (A) Appearance of bolt with three probes, as labelled prior to securing the probes or wrapping for transport. (B) Scout CT images (coronal and sagittal, respectively) demonstrating the trajectory of the probes approximately 1.5 cm (Depth) and 2-3 cm (ICP/PbtO2, rCBF) below the inner table of the skull. (C) Axial CT after non-surgical severe TBI with excellent placement. Notice with standard windowing that the relatively dense probes may obscure subtle peri-probe hematoma. (D) Axial CT after surgical severe TBI demonstrating the placement of the bolt and probes contralateral to the hemicraniectomy site. (E) Incorrect (deep) placement of the probes after non-surgical severe TBI. Note that the probes are approaching the frontal horn of the lateral ventricle, indicating they are >3 cm below the inner table of the skull. This placement may affect measurements obtained by the probes, although shallow, rather than deep, placement is more liable to create problems with rCBF and PbtO2 measurements. Please click here to view a larger version of this figure.
| Equipment | Measurement | Method of Measurement | Sampling Resolution |
| Quad lumen bolt kit | NA | NA | NA |
| ICP/PbtO2 probe | ICP | Mini-strain gauge | 125 Hz |
| PbtO2 | Fiberoptic | 125 Hz | |
| ICT | Thermistor | NA | |
| rCBF probe | rCBF | Distal thermistor | 1 Hz |
| ICT | Proximal thermistor | 1 Hz | |
| K | Distal thermistor | per recalibration | |
| Depth electrode | EEG | Platinum electrodes | ≥256 Hz |
| 70 Microdialysis bolt catheter | Lactate, pyruvate, glucose, glycerol, and glutamate | Enzymatic measurement of interstitial fluid | Hourly |
Table 1: Intracranial probes. The names of the probes used in this article and their measurements and sampling resolution. Please note that this is a representative list of probes that may be used for multimodality monitoring but does not represent an exhaustive list of the potential modalities that may be commercially available. EEG = electroencephalography; ICP = intracranial pressure; ICT = intracranial temperature; PbtO2 = brain tissue oxygen; rCBF = regional cerebral blood flow.
