Positron emission tomography/computed tomography (PET/CT) is a nuclear imaging technology that enables visualization of metabolic processes in the body following injection of a radioactively labeled ligand, also called tracer. Whereas the ligand is a molecule that is involved in a metabolic pathway or targets cell surface proteins, the radioactive label is a positron-emitting radionuclide. Gamma rays are indirectly emitted by the positron decay and allow the detection of its distribution in the organism with extracorporeal PET detectors. In this way, different cellular molecules can be targeted: neurotransmitter receptors and transporters, metabolic processes like glycolysis or mitochondrial proteins like the translocator protein 18 kDa (TSPO) to detect activated glia cells.
In preclinical research, PET/CT is an attractive method to study biochemical processes in a non-invasive manner in vivo, thus allowing longitudinal studies. PET/CT data support the analyses of disease mechanisms, the assessment of the characteristics and pharmacokinetics of new drugs and the validation of both, current and novel radiotracers for translational research.
During PET/CT analyses three tracer states can be defined (example of the 2-tissue compartment model): First, the tracer flows within the blood after its application (state 1; conc.[blood]). Second, it enters the tissue via the capillary bed and can there either freely move within the extracellular space or is unspecifically bound to diverse cellular or extracellular structures (state 2; conc.[unspec]). Third, the tracer can be specifically bound (with or without metabolic trapping) to its target molecule (state 3, conc.[spec]). All these dynamic processes between the compartments are to some extent bidirectional and the diffusion processes are described by rate constants (K1, k2, k3, and k4). While the concentration of the tracer in the blood (i.e., state 1) is called "Input", the concentration of unspecifically and specifically bound tracer (i.e., state 2 and state 3) is called "Output" and can be directly derived from the PET Image. This physiological relation can be displayed in the 2-tissue compartment model (Figure 1).
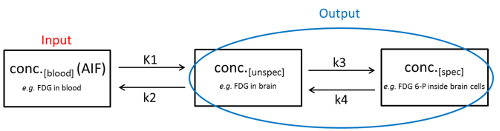
Figure 1: The two-tissue compartmental model. The physiological conditions of the three different tracer states and the dynamic processes between them are displayed. Please click here to view a larger version of this figure.
In the ideal case, conc.[spec] is proportional to the concentration of its target molecule. However, the output of the PET/CT measurement is the sum of conc.[spec] and conc.[unspec]. To determine conc.[spec] in the region of interest, in parallel the conc.[unspec] of a reference region devoid of the target protein/pathway is determined. By using appropriate mathematical equations one can now calculate conc.[spec], most commonly using the compartment model (a bio-kinetic modeling approach). However, in many cases, such a reference region devoid of the target protein is not available1,2. In these cases, the conc.[blood] can be used to determine conc.[spec]. Since the conc.[blood] is varying due to different liver and kidney clearance, excretion, blood flow, different brain-blood barrier penetration and disease-related factors3, the current gold standard is to measure the conc.[blood] in parallel to the PET/CT scan by continuous blood sampling. This gives the arterial input function (AIF), which is defined as conc.[blood] over time4. Of note, performing continuous blood sampling is considered technically highly challenging, especially in small animals such as rats or mice5.
Here, we provide an easy and practical protocol to continuously sample blood from rats via an arteriovenous (a-v) shunt between the femoral vein and artery. Coupled to a commercially available detector-pump system, we are able to generate a real-time, continuous AIF during dynamic [18F]fluorodeoxyglucose ([18F]FDG)-PET/CT scans in rats and compared it to alternative approaches. PET/CT imaging was performed in male sprague dawley rats at an age of 4 months with an average weight of 462 g ± 33 g (mean ± standard deviation) using a multimodality PET/CT scanner.
Since a wide variety of devices is used during the series of measurements (dose calibrator, online blood sampler, PET/CT, and well counter), a quality control procedure referred as cross calibration is needed to check the quantitative accuracy of all systems and to compensate for differences. Cross calibration in the context of online blood sampling means that the count rate for a given activity concentration measured in corrected PET images can be converted into the concentration measured with the twilite system for the same concentration. Therefore, a cross calibration procedure between PET/CT, blood sampling system, and well counter has been established.
This highly standardized methodology provides a powerful approach to quantify metabolic and cellular processes in preclinical small animal research and is an elegant way to improve the reliability and reproducibility of the AIF. The AIF can then be used to quantify the specifically bound tracer in tissue in preclinical PET/CT data using bio-kinetic modeling.
All animal handling and experiments were approved by the state Animal Research Committee of Mecklenburg–Western Pomerania (LALLF M-V/7221.3-1.1-004/18, approval: 03.04.2018). The experiments were performed in compliance with the ARRIVE Guidelines.
NOTE: Animals were kept under standard conditions (22 ± 2 °C, 12 h day-and-night cycle) with water and food ad libitum. All needed equipment for the preparation of the shunt system, the operation procedure and the actual measurements are listed in the Table of Materials.
1. Preparation and surgical procedure for catheterization of the animal
- Fast the animal for at least 12 h with free access to water. For anesthesia, place the rat in an induction chamber and fill it continuously with oxygen/isoflurane mix. For initiation use 2.5-3.5% isoflurane and for maintenance 1.5-3.0% (flow rate of 1.2-1.5 L/min).
NOTE: Fasting is necessary for studies using the tracer [18F]FDG but not for other tracers. Measuring glucose blood levels using manual blood draws described in section 4 is recommended to ensure stable values or to correct for in kinetic modeling. - Place the anesthetized rat in dorsal position on a heating mat, under the surgical microscope and add vet ointment on its eyes. Monitor and maintain the body temperature of the rat continuously during the experiment (37 ± 0.5 °C) with a rectal probe.
- Tape the legs of the rat to the work surface to hold the legs in position. Disinfect the operating site with a mucosal disinfectant and shave the leg and crotch (operation side) of the rat. Finish with a final cleansing with the disinfectant.
- Make an incision of about 20 mm using surgical forceps and scissors at the groin of the rat. Dissect the fine skin layers and expose the femoral vein, artery and nerve with the micro forceps. Place two fine filaments under each femoral vein and artery.
- Seal vein and artery with each distal filament and hold under tension with a bulldog clamp.
Use the proximal suture filaments to tension the vessel using the bulldog clamps (without a knot). - Block the vein with an aneurysm clamp proximal, but 2-3 mm distal from the suture with the bulldog clamp. Use corneal scissors to make a small incision into the vein (1/3 of the diameter) and remove leaking blood with a sterile cotton swap. Dilate the vein with a dull forceps and hold it open. Insert the sharpened catheter (inner diameter [ID]: 0.58 mm, outer diameter [OD]: 0.96 mm) into the vein and push it in proximal direction, up to the aneurysm clip.
- Open the aneurysm clip and push the catheter further in proximal direction (approximately 2-3 cm), if the catheter is placed right, blood will flow into the catheter. Secure the catheter with the proximal suture by making two knots; if necessary, place an additional suture around the vein and the catheter. Check the functionality of the catheter by flushing and aspirating with an insulin syringe (30 G needle) filled with 100 µL of heparinized saline solution (50 units/mL).
- Place the catheter in the artery by repeating steps 1.6 and 1.7.
- When both catheters are correctly placed, close the leg with sutures and carry the animal to the PET/CT.
NOTE: Be as careful as possible with the catheters during transport of the animal, otherwise shifting of the catheter might occur.
2. Setup of the shunt system
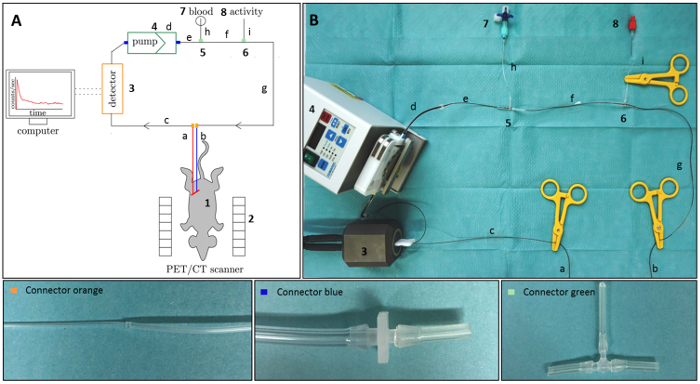
Figure 2: Scheme of the measurement setup. (A) Schematic drawing of the measurement setup. (B) Photo of the connected shunt system with the twilite detector, peristaltic pump and different connector types. The time-course of radioactivity in blood of a rat is detected while the animal (1) is scanned in the PET/CT (2). Therefore the arterial (a) and venous (b) catheter is connected to the detector pump system via adapter pieces (connector orange, connector blue and connector green). The arterial blood is then pumped from the arterial catheter through the detector (3) to a peristaltic pump (4) and back into the body via the venous catheter. A 3-way valve (7) is integrated in the tube system to perform tracer injection, manual blood draws and rinsing. A T-piece (8) is assembled to inject activity. The detector is connected with a computer to view, calibrate and correct the continuous blood data. Please click here to view a larger version of this figure.
- Cut off 6 parts of the fine bore polythene tubing (FBPT) (ID: 0.58 mm, OD: 0.96 mm) with a length of c = 735 mm; e = 100 mm; f = 171 mm, g = 875 mm; h = 90 mm and i = 75 mm (Figure 2). Cut off 8 parts of the silicone pump tubes (black/black/black, ID: 0.76 mm, OD: 2.48 mm) with a length of approximately 20 mm.
- Place reduction connectors (from ID 2.5 mm to ID 1.5 mm) on both ends of the silicone pump tube d (yellow/blue/yellow, ID: 1.52 mm, OD: 3.20 mm). Put a prepared 20 mm part of the silicone tubes (black/black/black) on the other end of the used reduction connectors (see connector blue in Figure 2).
- Place the prepared part c of the FBPT in the assembled connector blue on the one end of the silicone pump tube d (yellow/blue/yellow) and the prepared part e of the FBPT in the assembled connector blue on the other end. Put a prepared 20 mm part of the silicone tubes (black/black/black) on the ends of two T-pieces 5 and 6 (tube T-connector ID: 1.5 mm; see connector green in Figure 2).
- Connect the free end of part e of the FBPT to the left side of the assembled connector green (5) and place the prepared part f of the FBPT at the opposite side of connector green (5). Place the free end of part f of the FBPT in left side of assembled connector green (6) and place the prepared part g of the FBPT at the opposite side of connector green (6). Add the prepared part h of the FBPT to the free end of the assembled connector green (5) and the prepared part i of the FBPT to the free end of the assembled connector green (6).
- Connect a combi-stopper to a hypodermic needle (G 23 x 1 1/4''/ø 0.60 mm x 30 mm) and add it to a three-way valve. Place the prepared three-way valve with the needle in the free end of the part h of the FBPT. Connect a combi-stopper to a hypodermic needle and place the needle in the free end of the part i of the FBPT.
NOTE: Before starting the online blood sampling, see section 5. - Put the free ends of part c and g of the FBPT into a 100 mL beaker filled with 20 mL of heparinized saline solution (50 units/mL). Start the peristaltic pump with a flow rate of 1.52 mL/min so that the shunt system is completely filled with the physiological saline solution. Afterwards set three scissor clamps at the ends of part c and g and in the middle of part i of the FBPT.
- Release the scissor clamps from part c and g of the FBPT. Connect the arterial catheter a to the free end of part c of the FBPT and connect the venous catheter b to the free end of part g of the FBPT (see connector orange in Figure 2).
3. Image acquisition and reconstruction
- Place the animal in head-prone position on the shuttle bed pallet (70 mm). Control respiration of the rat and keep body temperature at 37 ± 0.5 °C using a heating pad and a rectal probe throughout image acquisition. Move the shuttle bed to the extended bed position for injection (pre-acquisition) and connect the inserted catheters to the shunt system.
- Keep the animal under anesthesia with isoflurane (2.5% isoflurane in oxygen, flow rate 1.2-1.5 L/min) via a nose cone.
- Start the peristaltic pump with a flow rate of 1.52 mL/min to fill the shunt system with the blood of the animal. Move the shuttle bed to the center of the field of view of the PET detection ring and start the online blood sampling system (see section 5).
- Start the PET/CT workflow using parameters described in section 3.5 after 60 s and subsequently inject a dose of approximately 22 MBq [18F]FDG in a volume of about 0.5 ± 0.1 mL intravenously via the T-piece. Flush the T-piece with about 150 µL of heparinized saline solution afterwards.
- Acquire a dynamic PET over 60 min and a CT scan at the end of the PET imaging.
- For PET emission acquisition, set 3600 s (60 min) in the acquire by time option. Select F-18 as study isotope and use 350–650 keV as energy level and 3,438 ns as timing window.
- For CT acquisition, select attenuation scan in the acquisition option. In the projection settings field, choose 120 projection for a half total rotation. For field of view (FOV) and resolution settings, select low as magnification and 4 x 4 as binding with 275 mm axial scanning length and 3328 px as transaxial CCD size. In the exposure settings field, set 500 µA for current, 80 kV for voltage and 180 ms for exposure time.
- For PET emission histogram, set a series of 20 frames (6 x 10 s, 8 x 30 s, 5 x 300 s and 1 x 1800 s) as dynamic framing. Select subtract as delays. Choose in the advanced settings field 128 as sinogram width, 3 as span, 79 as ring difference and dead time correction.
- For PET reconstruction, use two-dimensional ordered subset expectation maximization (2D-OSEM) with a generate, apply and save scatter sinogram, 4 iteration and Fourier for rebinning as reconstruction algorithm. Select 128 x 128 as matrix size and use 1 as image zoom, all as frames and all as segments.
4. Procedure of manual blood sampling
- Perform manual blood sampling 30 s, 60 s, 90 s, 600 s and 1800 s after starting the imaging acquisition.
NOTE: Increasing the number of manual blood draws especially within the first minute after tracer injection is highly recommended if possible. Therefore the blood sample volume has to be reduced to 20-30 µL per sample6.- Open the first three-way valve and collect 100 µL of arterial blood into a capillary blood collection EDTA tube 30 s after tracer injection. Repeat for the other time points. Determine the weight of the empty tube and blood filled tube.
- Measure the activity (counts/time unit) of the whole blood for 180 s in a well counter, which is later cross calibrated to obtain data in kBq/mL. Record the start time of the well counter measurement. Calculate the activity of whole blood for each time point of the manual blood sampling in kBq/mL, apply decay correction and transfer the data in a time activity curve.
5. Procedure of the online blood sampling
- Place the tube into the detector using the tube guide. Start the blood sampler software (e.g., PSAMPLE) and open the acquisition interface. Ensure that the computer of the online blood sampling setup and of the PET/CT is time synchronized.
- Press the start button exactly 60 s before the tracer is injected to acquire enough data for background correction. Save the raw data via the save button in the PMOD database after the measurement.
- For correction and calibration of the online blood data, switch to the correction interface. Enable the decay correction and select 18 F. Define the start time of image acquisition and enable the average button to perform background correction. Activate the calibration and type in the previously determined calibration factor (see section 7.1).
- Save the corrected and calibrated blood data using the save TAC button and choose the file blood.crv. This file can then be loaded as whole blood input curve into the kinetic modeling tool and kinetic modeling can be performed. Decouple the catheters from the extra corporal shunt system.
- Detach the animal from the PET/CT scanner and euthanize with pentobarbital.
NOTE: In this experiment, animals were euthanized after the measurements as brains were used for in vitro analyses in the experimental design. With this setup, repeated measurements in longitudinal studies are also implementable7. Use a completely new tube system for the next animal.
6. Image derived Input function
- Open the Fuse it tool on PMOD. Load the PET Image as input and the CT as reference. Click already matched.
- Open the voxel of interest (VOI) tool. Place the cursor within the ascending aorta in the CT. Click predefined spherical VOI. Define a radius of exactly 0.7 mm. Extract the time activity information with the VOI statistic button and copy the averaged values to clipboard.
7. Procedure of cross calibration of the twilite system, PET/CT and well counter
- Twilite-PET/CT-calibration
NOTE: The presented workflow for calibration of the twilite is partly based on the procedures described in the reference manual of the PSAMPLE module of PMOD.- Fill a syringe with approximately 100 MBq of [18F]FDG. Measure the exact activity AF with a calibrated dose calibrator and document it together with date and time of the measurement and the volume of the full syringe. The recorded time is the reference time point for all decay corrections to be performed.
- Fill a beaker with 500 mL of tap water. The exact volume is determined by the weighing method. Measure the weight me of the empty beaker with an appropriated and calibrated precision scale (at least accuracy class II). Fill the beaker with the tap water and measure the weight mf of the full beaker.
- Calculate the volume Vb of the beaker by using the difference of the mass and the density of tap water (r = 0.998 g/mL at 20 °C):

- Inject the [18F]FDG into the filled beaker and refill the empty syringe to its original volume with inactive tap water and measure the activity AE of the refilled syringe in the dose calibrator. The activity concentration cb of the solution in the beaker is given by
 , which should be approximately 200 kBq/mL.
, which should be approximately 200 kBq/mL. - Fill a 50 mL conical centrifuge tube with the solution from the beaker (avoid large air bubbles) and place it centrally in the field of view of the PET/CT scanner. Fill a catheter identical to the type used in the PET/CT imaging experiment and place it in the tube guide of the twilite system. Fill the catheter with the tracer solution from the beaker using the peristaltic pump.
- Start the measurement of the time activity curve as described in section 5, using the same parameter for integration time, and rebinning as in the experiment, without a catheter guide inside the measurement head. This step ensures the acquisition of enough data for appropriate background correction. After 2 min, without stopping the data acquisition of the twilite system, place the catheter guide with the filled tube into the measurement head, and continue the data acquisition for about 5 min.
- Start a 10 min PET acquisition of the 50 mL conical centrifuge tube in parallel followed by a standard CT acquisition for attenuation correction. Reconstruct a static PET image of the 50 mL conical centrifuge tube using the same PET reconstruction algorithm and parameters described in section 3. Use a post processing imaging tool (e.g., PVIEW) and place a cylindrical VOI covering approximately 70% of the volume inside of the reconstructed PET images of the 50 mL conical centrifuge tube. Extract the mean activity concentration cPET in kBq/mL within the VOI.
- Go back to the blood sampler software and use the calibration mode to correct the acquired TAC for decay, branching fraction and background. Add all the necessary information for nuclide, activity concentration and the PET acquisition start time. Internally, the software extracts the count rate measured with the twilite system (CRtwilite) and calculates the cross calibration factor for PET and twilite system (CFPET/twilite):
NOTE: It is important that the same isotope is used for both calibration and PET/CT experiments, as the branching fraction varies between the different isotopes, which is corrected for in the PET reconstruction process. This procedure has to be repeated regularly in terms of quality control, if important components of the system are changed (e.g., tubes, acquisition and reconstruction parameters) and after repair works.
- PET/CT-well counter calibration
- To calculate the calibration factor CFwell-counter of the well counter, use the same activity solution that has been produced in the beaker for the calibration of the twilite system. Wait approximately 6 h to allow reduction of specific activity by decay to minimize dead time effects of the scintillation detector of the well counter. Lid the beaker to avoid evaporation.
- Calculate the exact time difference to the reference time point and determine the actual activity concentration cb(t+) of the solution of the beaker by decay correcting the original activity concentration . Pipette predefined volumes (Vsample) that are identical to the volume of the blood samples measured within the experiments (e.g., 200 µL), from the beaker into five safe-lock tubes. Measure the activity of each of the five tubes with the well counter for 180 s.
NOTE: If the coefficient of variation for a single measurement is greater than 1%, the measurement time should be increased. Record the measured count rate in counts per minute [cpm] for each tube and the measurement start time. Perform a decay correction. - Calculate the calibration factor CFwell-counter for each measurement by dividing the decay corrected count rate CRwell-counter of the well counter by the decay corrected activity concentration of the beaker cbeaker(t+):

- Average the five calibration factors to obtain the mean calibration factor.
The setup of the shunt system is displayed in Figure 2. Representative results of the continuous blood sampling data compared to manual blood sampling data in three wildtype rats over a time span of 30 min are presented in Figure 3A,C. At the beginning of the continuous blood sampling, an initial peak (maximum of radioactivity concentration) can be seen at 5 s after tracer injection. Afterwards, the activity in the blood declines rapidly and reaches a plateau at about 15 min. In the manual blood sampling data the detected Peak is smaller and the plateau is not easily to define (Figure 3A,C). The comparison of the continuous blood sampling to the image-derived data is displayed in Figure 3B,D. In the image-derived data, the peak and the starting point of the plateau are clearly visible, nevertheless the maximum of the peak is smaller compared to continuous blood sampling data for all animals (Figure 3B,D).
A sub-optimal outcome of continuous blood sampling with our setup is shown in Figure 3E,F. At the beginning of the continuous blood sampling, no data acquisition within the first 3.5 min was possible due to blood clotting. By disconnecting the tube system at connector orange and floating with heparinized saline solution, the flow in the tube system was restarted and the measurement continued. A peak can be seen at about 4 min, which does not record the maximum of radioactivity in blood (Figure 3E,F). Manual blood sampling (Figure 3E) and image-derived analyses (Figure 3F) were still possible and comparable to the correct outcomes.
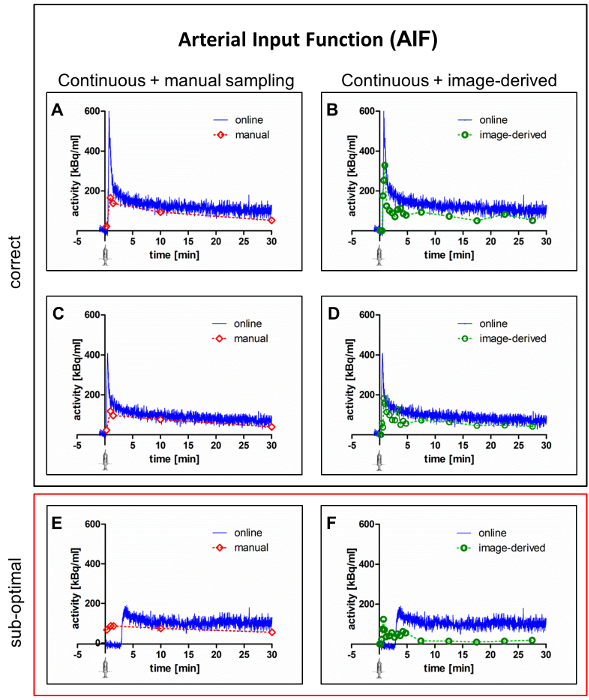
Figure 3: Representative results of continuous blood sampling compared to manual blood sampling. Typical arterial input functions derived from continuous blood sampling compared to manual blood sampling (left column) and continuous blood sampling compared to the image-derived approach (right column) are shown. Panels A-D demonstrate the results of correct implementation of the protocol in two different animals. Panels E and F illustrates a sub-optimal outcome of the measurement. All data shown were corrected for the cross-calibration factor and the background. Please click here to view a larger version of this figure.
