Using the methods described, we were able to collect over 700 days of data and over 3,000 PVTs and fatigue ratings among 44 short-haul pilots7. The goal of this study was to characterize changes in sleep, circadian phase, fatigue ratings, and performance among short-haul pilots by work start-time and workload during daytime flights.
To account for the within-subjects study design, all condition effects were evaluated for sleep and performance outcomes using repeated measures analysis of variance with unstructured covariances, using participant as a repeated factor. To evaluate whether sleep and performance outcomes varied by day on a given schedule, linear mixed effects models were applied to the changes in sleep and performance by day. To account for individual differences in adaptation to a given schedule, the intercept and slope were allowed to vary by individual.
The first objective addressed with these methods was to examine the impact of duty start time on sleep. Sleep duration, bedtime, wake time, and sleep quality were calculated using the sleep diary and actigraphy. An example of the actogram derived from activity monitor is illustrated in Figure 7. It was demonstrated that sleep timing and duration varied significantly as a function of work start time using mixed-effects regression analysis. Table 1 displays the bedtime, wake time, sleep duration and sleep quality by schedule type as reported by participants in the sleep diary. Participants went to bed on average at around 23:10 (SD = 1:41) on baseline block. The bedtime for early duty schedule block differed significantly from baseline (p < 0.01) with participants reporting earlier bedtimes. The bedtimes for mid-day and late duty schedules also differed significantly from baseline (p < 0.01), with participants reporting later bedtimes. Participants went to bed significantly later (p < 0.01) on rest days compared to baseline.
Figure 8 displays the mean-actigraphy derived sleep duration by day for each schedule type. Participants obtained significantly less sleep (p < 0.01) on early starts compared to baseline. The sleep duration on the other schedule types were not different from baseline. Sleep latency and sleep efficiency obtained from actigraphy were not significantly different from baseline for any of the schedule types. Wake after sleep onset (WASO) was significantly different for early starts compared to baseline (p < 0.05), with pilots reporting being more awake during the early starts. There were no differences between the baseline and other schedule types. There were no significant differences between rest days and the baseline.
The second objective addressed with these methods was to examine the impact of duty start time on circadian phase as measured by aMT6s. The peak timing (acrophase) of the aMT6s rhythm is a reliable marker of circadian phase58. Figure 9 shows an example of the circadian rhythm of aMT6s over 24 h for one individual, while Figure 10 shows the aMT6s acrophase for each individual who participated in the urine collection procedures by study block. Consistent with the findings on sleep, it was found that mean circadian phase was significantly shifted according to work start time. It is important to note the missing data collection information in Figure 10. Some individuals had difficulty with the urine collection procedures for some of the blocks or they forgot to log the timing of their sample collection. In these cases, it was not possible to generate reliable estimates of circadian phase from the aMT6s concentration and as a result some data are missing. In situations where collection of circadian phase information is important, it may be prudent to call participants prior to each urine collection to ensure the procedures are properly followed.
The third objective addressed with these methods was to examine the impact of duty start time on self-reported fatigue as measured by SP, and objective performance as measured by the PVT. Consistent with our findings with sleep, using mixed-effects regression analysis, we found that both fatigue (Table 2) and PVT reaction times (Figure 11) were worse during early starts, high workload mid-day shifts, and late finishes, relative to our baseline data collection (p < 0.001 SP; p < 0.01 PVT RT). Participants showed a significant increase in lapses for each schedule type compared to baseline (p < 0.01 early; p < 0.05 mid-day; p < 0.01 late). Performance on rest days was similar to that of the baseline. These results are also described in Table 3.
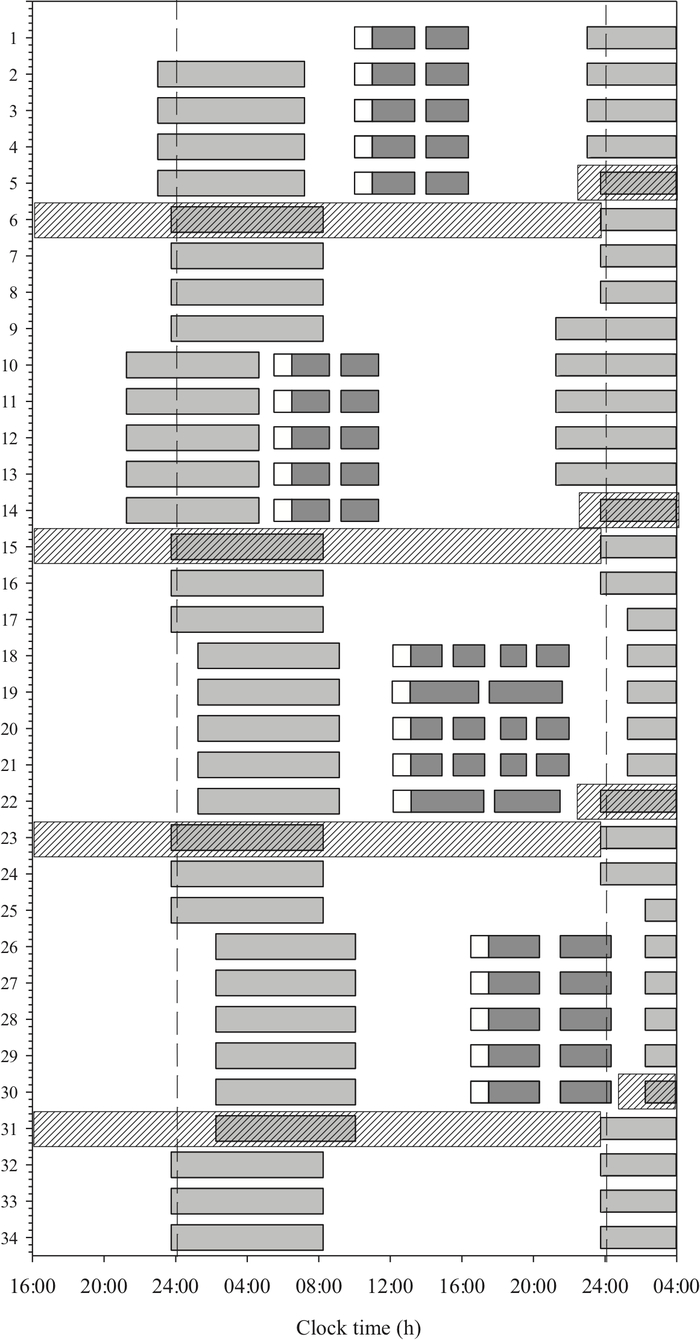
Figure 1: Study protocol by time of day for each day of the study. The dark gray bars represent the flight periods including the pre-flight report time (open bars), and the light gray bars represent the sleep periods. Days 1–5 represent the baseline duty block, days 10–14 represent the early duty starts, days 18–22 represent the mid-day duty starts, and days 26–30 represent the late starts. The shaded bars represent the first rest day post duty block when urine is collected. This figure is reproduced from Flynn-Evans et al.7. Please click here to view a larger version of this figure.

Figure 2: The activity monitor/accelerometer device worn on the wrist of the non-dominant hand. Please click here to view a larger version of this figure.
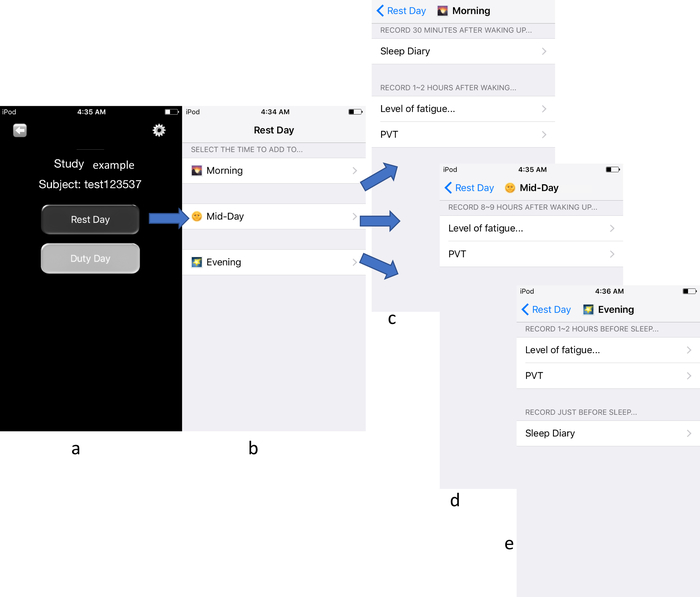
Figure 3: Example of tests taken during rest days using the touchscreen application. From left to right: (A) the main page of the app displays two links; (B) the rest day displays three links: morning, mid-day, evening; (C) the morning link displays the tests taken in the morning; (D) the mid-day link displays the tests taken in the afternoon, and (E) the evening link displays the test taken in the evening. Please click here to view a larger version of this figure.
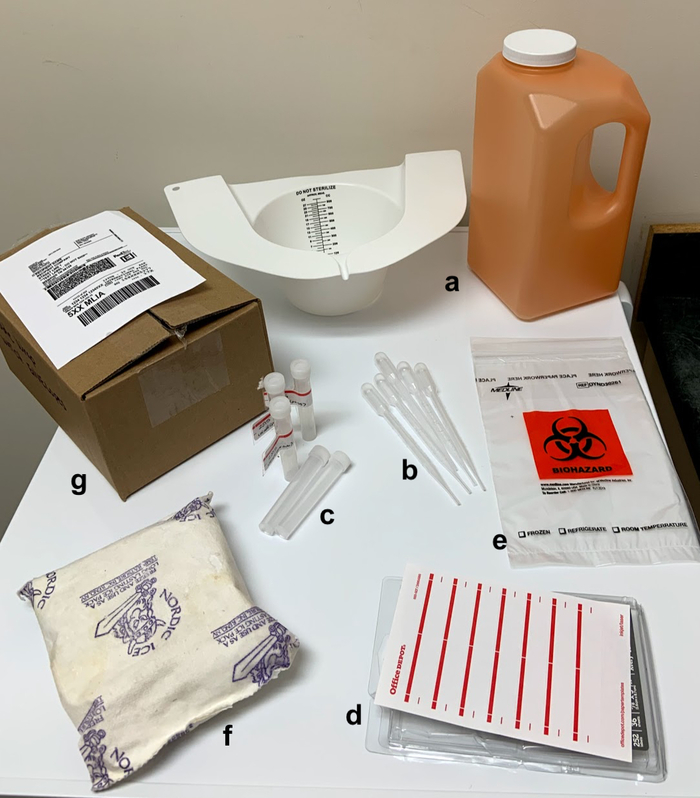
Figure 4: Urine kit. The kit contains (A) a urinal hat or urinal collection container, (B) pipettes, (C) urine collection tube, (D) white sticker labels, (E) a bio-hazard bag, (F) ice pack, and (G) shipping materials. Please click here to view a larger version of this figure.
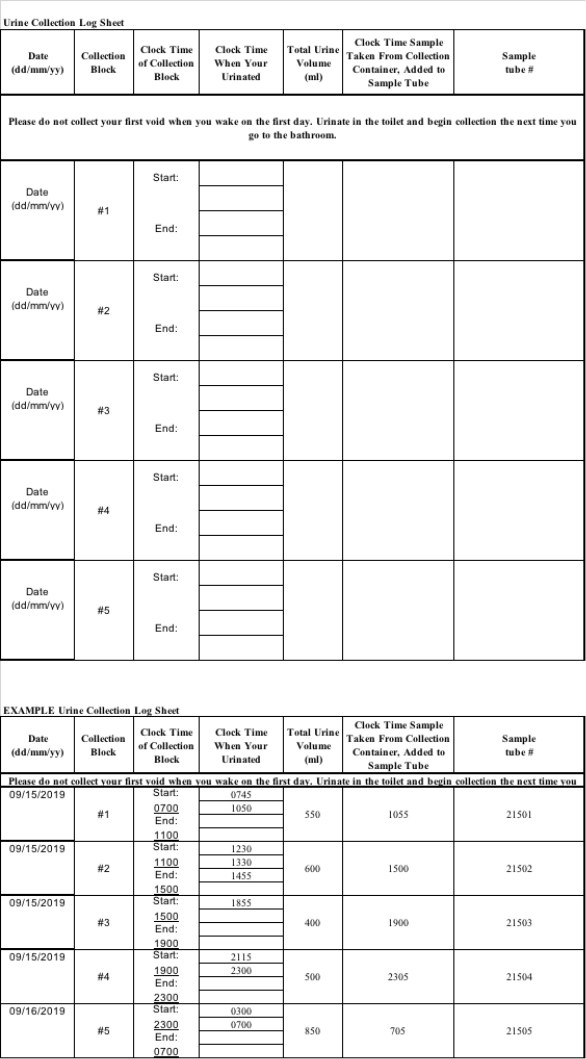
Figure 5: Example of the urine collection log.
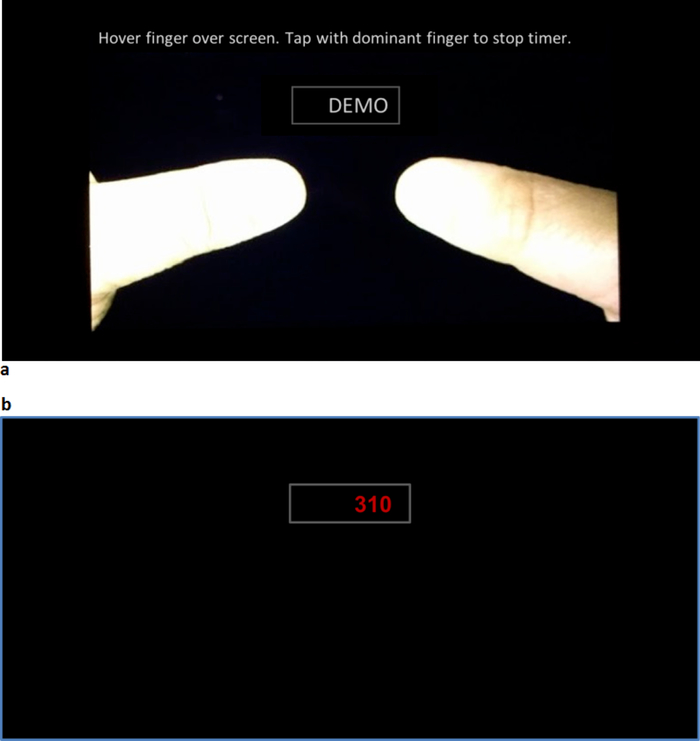
Figure 6: Psychomotor Vigilance Task (PVT). (A) The touchscreen device is oriented in landscape position and the thumbs are displayed on the screen at the beginning of the test. (B) the reaction times are displayed on a rectangular box in the upper middle part of the screen. Please click here to view a larger version of this figure.
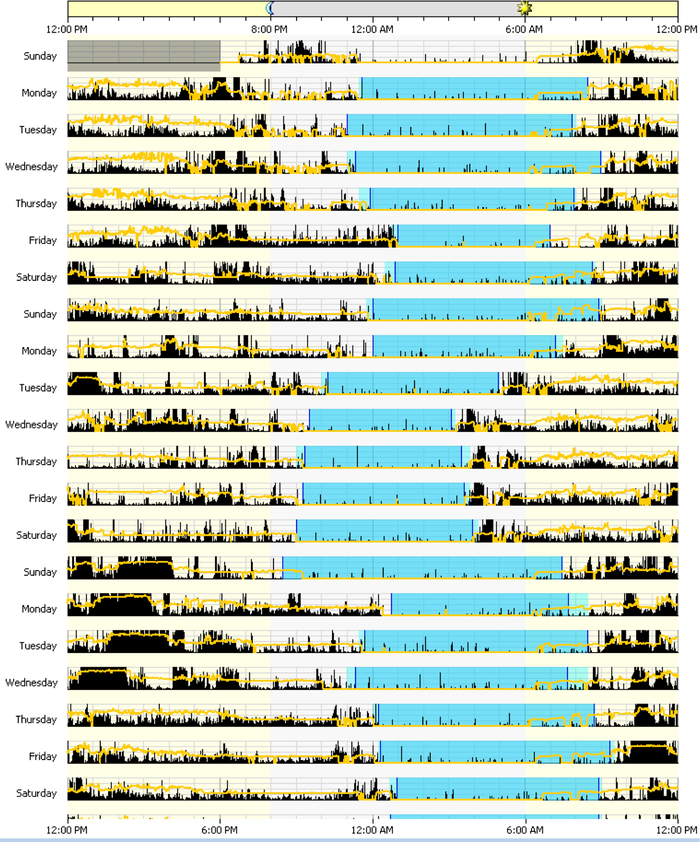
Figure 7: Actogram of sleep-wake cycles over 24 h for 14 days. The dark blue color represents the sleep periods; the light blue represents the rest periods. The black color represents movement. The yellow color represents the light. Please click here to view a larger version of this figure.
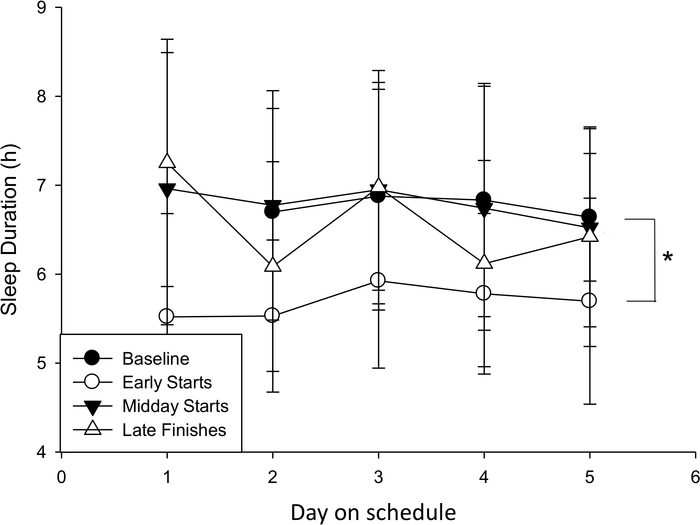
Figure 8: Mean actigraphy-derived sleep duration by day on each schedule type. Day 1 represents the night of sleep before the first work period of a given block. An asterisk designates a significant difference (*p < 0.05, **p < 0.01) in the means between the baseline condition and early starts block. Please click here to view a larger version of this figure.
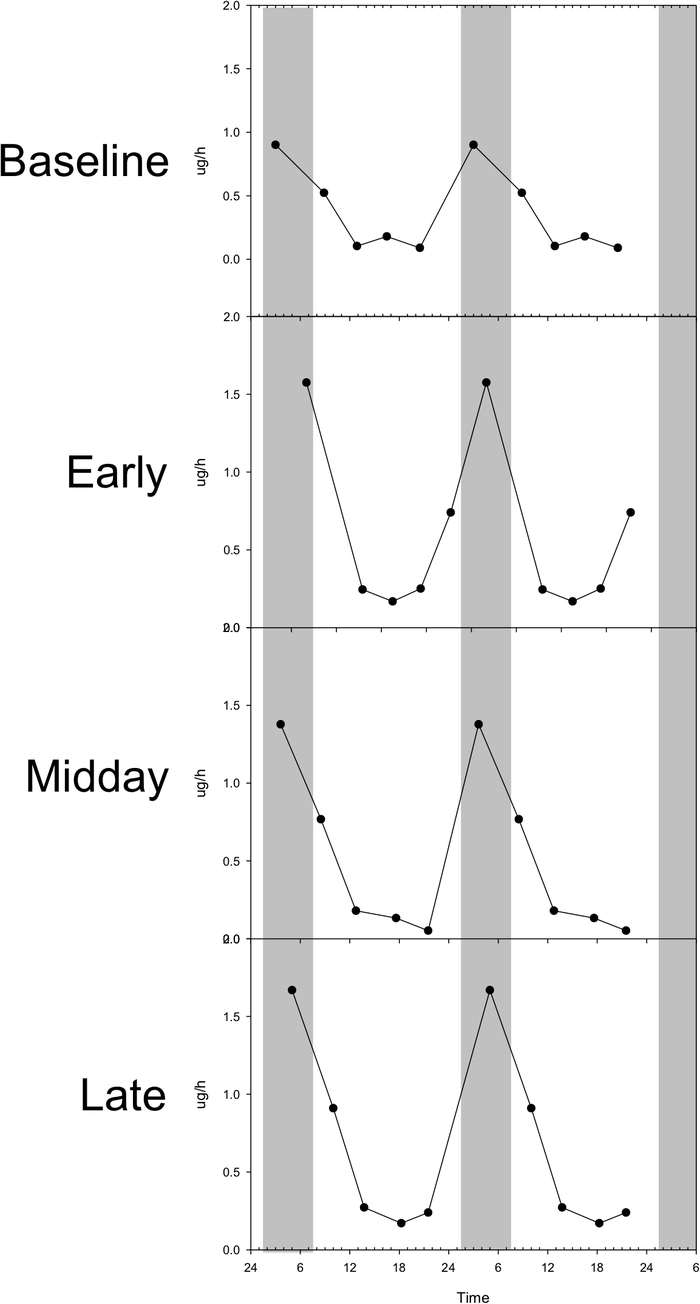
Figure 9: aMT6 profile for the five urine collection bins for each data collection episode for a single participant. Data are double-plotted. Please click here to view a larger version of this figure.
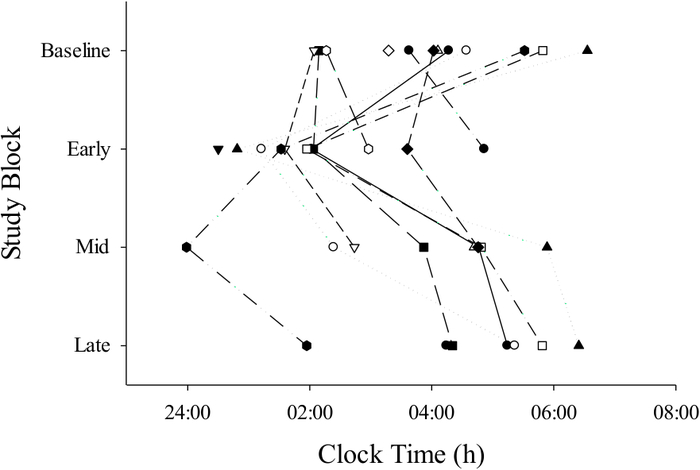
Figure 10: 6-sulfatoxymelatonin (aMT6) acrophase (peak) by time (24 h clock) of circadian nadir and schedule type for each individual. Filled and open circles, triangles, squares represent individual participants. This figure is reproduced from Flynn-Evans et al.7 Please click here to view a larger version of this figure.
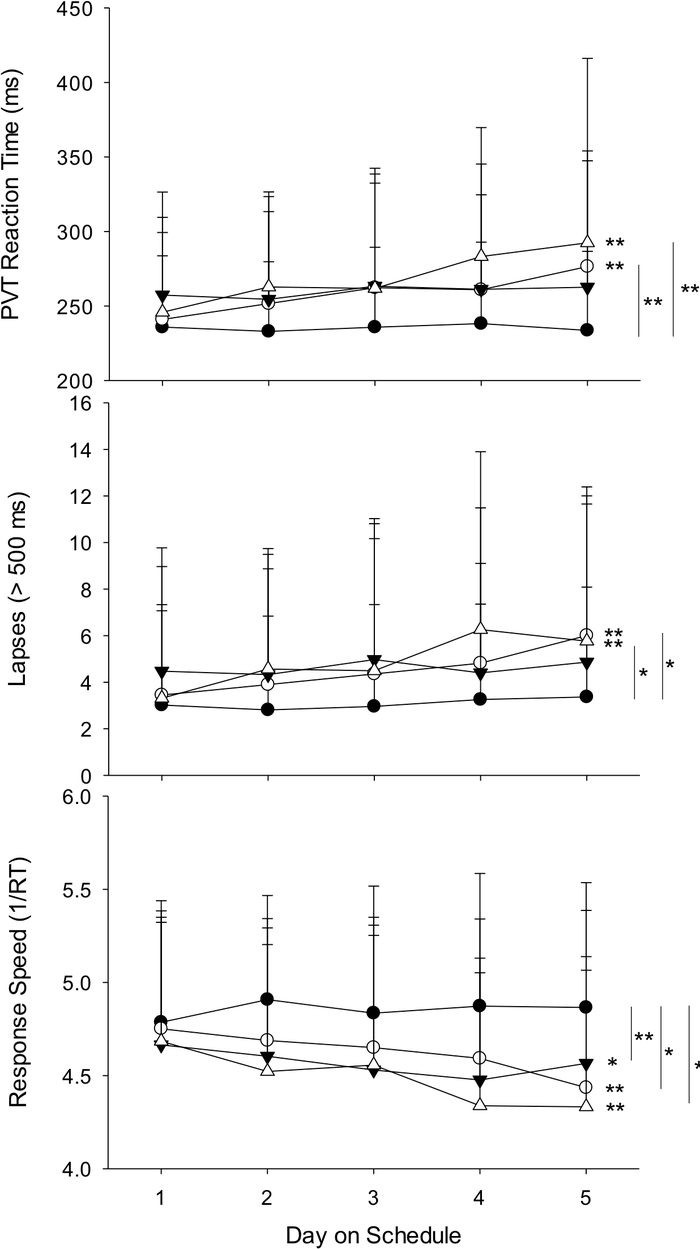
Figure 11: Psychomotor Vigilance Task (PVT) mean reaction time (RT), lapses (RT >500ms), and response speed (mean 1/RT) by day on each schedule type. Asterisks following each slope indicate changes in performance by day in that condition. Brackets indicate differences in the slope between baseline performance and the slope in performance in each of the other conditions (*p < 0.05, **p < 0.01). Baseline = filled circles, early = open circles, mid-day = filled triangles, late = open triangles. Please click here to view a larger version of this figure.
| Work schedule | n | Bedtime (h, SD) | Wake time (h, SD) | Sleep duration (h, SD) | Sleep quality (SD) |
| Baseline (ref.) | 39 | 23:10 (1:41) | 7:20 (1:49) | 8.2 (0.9) | 2.4 (0.7) |
| Early | 42 | 21:14 (1:01)** | 4:29 (0:47) | 7.4 (0.9)** | 2.5 (0.6) |
| Midday | 41 | 01:19 (0:43)** | 9:11 (0:58) | 7.9 (1.1) | 2.3 (0.6) |
| Late | 40 | 02:18 (1:07)** | 9:57 (1:11) | 7.8 (1.4)* | 2.3 (0.7) |
| Rest days | 42 | 23:47 (0:50)** | 8:16 (0:58) | 8.5 (0.9)* | 2.4 (0.5) |
Table 1: Sleep diary-derived sleep outcomes (bedtime, wake time, sleep duration and sleep quality) by schedule type. *p < 0.05, **p < 0.01; h = hour, SD = standard deviation. This table is reproduced from Flynn-Evans et al.7
| Work schedule | Mean (SD) | p-value |
| Baseline | 3.51 (0.80) | ref. |
| Early duty | 4.03 (0.88) | < 0.001 |
| Midday duty | 3.85 (0.90) | < 0.001 |
| Late duty | 3.85 (0.89) | < 0.001 |
Table 2: Means and standard deviation for Samn-Perelli (SP) scores by duty block. A higher rating indicates greater fatigue.
| Work schedule | n (participants) | Mean reaction time (ms, SD) | Response speed (s, SD) | Mean Lapses (> 500 ms) |
| Baseline (ref.) | 38 | 236 (48) | 4.84 (0.61) | 3.1 (4.1) |
| Early | 40 | 257 (70)** | 4.63 (0.66)** | 4.4 (5.4)** |
| Midday | 39 | 261 (62)** | 4.56 (0.66)** | 4.7 (5.1)* |
| Late | 38 | 266 (64)** | 4.51 (0.63)** | 4.7 (5.0)** |
| Rest days | 40 | 249 (56) | 4.69 (0.62) | 4.0 (4.5) |
Table 3: Psychomotor Vigilance Task (PVT) mean reaction time (RT), response speed (mean 1/RT), and lapses (RT > 500 ms) by schedule type. *p < 0.05, **p < 0.01; this table is reproduced from Flynn-Evans et al.7
