Results and figures presented here are referred to CF embryos generated through the injection of cftr morpholinos as described previously10 and in step 5. To validate the CF phenotype, the impaired position of internal organs such as heart, liver, and pancreas as previously described17 (Figure 1) were considered. Similar results were obtained in case of the WT embryos as reported in our previous publication19.
Bacterial burden was reduced by phage therapy in CF embryos infected with PAO1. Furthermore, we evaluated the bacterial burden at 8 hpi by homogenizing groups of 15 embryos: the average number of bacteria (cfu/embryo) present in the PAO1 infected embryos was reduced to about 20% after phage administration treatment, thus confirming a less severe infection in the presence of the phage cocktail (Figure 2).
Lethality was reduced by phage therapy in CF embryos infected with GFP+ bacteria PAO1. CF zebrafish embryos at 48 hpf were injected with GFP+ bacteria of the PAO1 strain at a dose that caused 50% lethality after 20 hpi (30 cfu/embryo, Figure 3A). The site of injection was the yolk or the Duct of Cuvier to generate a systemic infection. Phage therapy against PAO1 infection was tested by injecting 2 nL of the equally mixed phage cocktail (300-500 pfu/embryo). The injection was performed at two different time points: 30 min (early) and 7 hours (late) after bacterial injection. In both cases, lethality was reduced at 20 hpi, indicating that phage therapy is effective (Figure 3B).
With live imaging, using a fluorescent stereomicroscope, we also followed the progression of the infection in CF embryos injected with GFP+ PAO1 and showed the efficacy of phage therapy in reducing the spread of fluorescent bacteria over the yolk sac. The CF+PAO1 injected embryo with GFP+ bacteria multiplication at 4, 9, 14 and 18 hpi is shown in the upper side of Figure 4, whereas the CF+PAO1+phages embryo with reduced fluorescence due to phage action against bacteria is shown in the bottom part (Figure 4).
Phage therapy reduced the inflammatory response generated by PAO1 infection in CF embryos. We, also, evaluated the immune response generated by PAO1 and PAO1 + phages injection at 8 hpi. As expected, the expression of the pro-inflammatory cytokines TNF-a and IL-1β analyzed by qPCR techniques was significantly increased following PAO1 injection in comparison to controls, while it was reduced with the co-injection of the phage cocktail (Figure 5A,B).
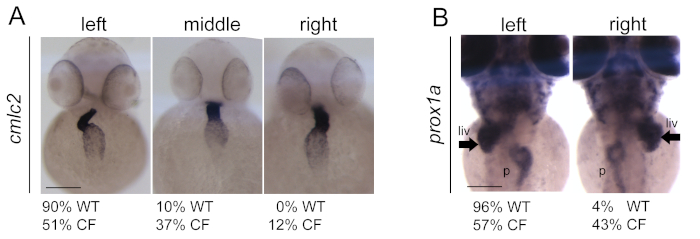
Figure 1: Generation and validation of CF embryos upon cftr morpholinos (cftr-MOs) injection. (A) Impaired position and looping of the heart in CF injected embryos in comparison to wild-type (WT) embryos. Heart is visualized with cmlc2 expression by in situ hybridization technique. (B) Impaired position of the liver (arrows) and pancreas in CF embryos in comparison to WT. Liver and pancreas are visualized with prox1a expression by in situ hybridization techniques. Scale bars indicate 100 μm. liv: liver; p: pancreas. The figure is reprinted from19 Please click here to view a larger version of this figure.
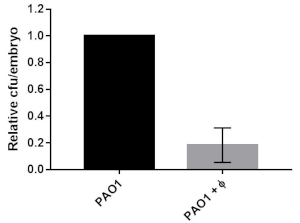
Figure 2: Bacterial burden in CF embryos infected with PAO1 or PAO1+phages. The relative percentage of cfu/embryo in PAO1+phages vs PAO1 embryos are given. The mean and SD of three independent experiments is reported. The figure is reprinted from19. Please click here to view a larger version of this figure.
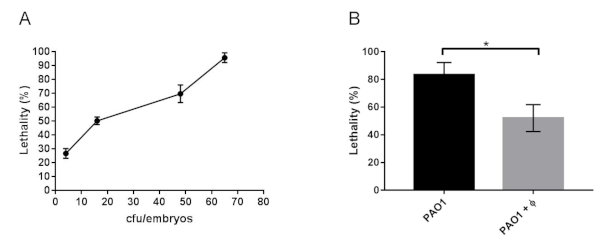
Figure 3: Lethality of CF zebrafish embryos infected with PAO1 and with PAO1+phages. (A) Determination of LD50 in 48 hpf zebrafish embryos microinjected with cftr-MO at 1-cell stage (CF embryos) and infected at 48 hpf with 2 nL of a culture of PAO1 containing increasing number of bacteria (cfu/embryo). Lethality of the embryos was observed at 20 hpi. (B) Lethality at 20 hpi of CF embryos infected with PAO1 at 48 hpf and treated with the phage cocktail (PAO1+ Φ). The mean and SD reported are from six and four experiments, respectively, each with 25-40 embryos. Angular transformation was applied to the percentage of lethality and one-way ANOVA followed by Duncan’s test was used. The figure is reprinted from19. Please click here to view a larger version of this figure.
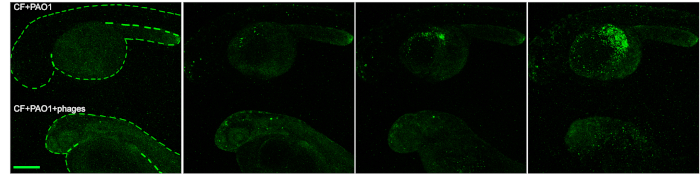
Figure 4: Imaging of the efficacy of phage therapy in zebrafish. Progression of the infection in CF embryos following PAO1 injection (upper embryo) and efficacy of the phage therapy in PAO1+phages injected embryos (bottom embryo) at 4, 9, 14 and 18 hpi. Scale bar indicates 100 microns. The figure is reprinted from19. Please click here to view a larger version of this figure.
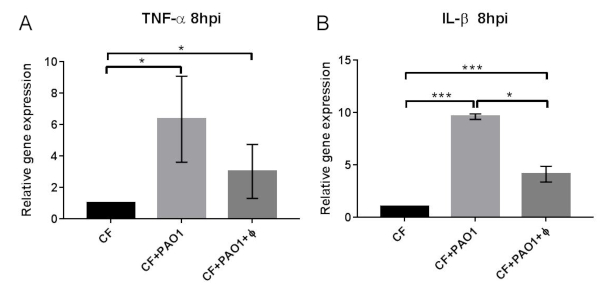
Figure 5: Expression of pro- and anti-inflammatory cytokines following PAO1 and PAO+phage administration. Expression levels of the TNF-a (A) and IL-1β genes measured by RT-qPCR at 8 hpi in CF embryos injected with PAO1 and PAO1+Φ at 48 hpf and normalized using the expression of rpl8. The mean and SD of four experiments are reported. Statistical significance was assessed by ANOVA followed by Duncan’s test: for TNF- a (CF) vs (CF+PAO1) p = 0.015*; (CF) vs (CF+PAO1+Φ) p = 0.019*; (CF+PAO1) vs (CF+PAO1+ Φ) p = 0.77 n.s.; for IL-1β (CF) vs (CF+PAO1) p = 0.00014***; (CF) vs (CF+PAO1+ Φ) p = 0.00068***; (CF+PAO1) vs (CF+PAO1+ Φ) p = 0.031*. The figure is reprinted from19. Please click here to view a larger version of this figure.
| Solutions | Preparation |
| Anaesthetic stock solution 25X | 4 mg/mL of Tricaine in distilled H2O. |
| Anaesthetic working solution 1X | dilute in distilled H2O the Tricaine stock solution 25X preparation to reach the 1X concentration (0.16 mg/mL) Tricaine of distilled H2O. |
| CsCl d=1.3 | 20.49 g in 50 mL TN |
| CsCl d=1.4 | 20.28 g in 50 mL TN |
| CsCl d=1.5 | 34.13 g in 50 mL TN |
| CsCl d=1.6 | 41.2 g in 50 mL of TN |
| E3 embryo medium for zebrafish embryo | 1 L 1of E3 (dilute the 50X stock with distilled H2O) + 200 μl of 0.05% methyl blue . Store at RT. |
| E3 embryo medium stock solution (50X) | 73.0 g NaCl, 3.15 g KCl , 9.15 g CaCl2 , and 9.95 g MgSO4 in 5 L of distilled H2O. Store at RT. |
| LB agar | 10 g/L tryptone, 5 g/L yeast extract, 5 g/L NaCl, 10 g/L agar |
| LB broth | for 1L: 950 mL H2O, 10 g Tryptone, 10 g NaCl, 5 g Yeast extract |
| PBST | PBS 1X + Triton X 1% |
| Physiological solution | 0.9% NaCl |
| Pigmentation blocking stock solution 10X | 0.3 mg/mL phenyl thiourea (PTU) powder in E3 embryo medium for zebrafish embryo |
| Pronase stock solution 5X | 5 mg/mL pronase powder in E3 embryo medium for zebrafish embryo |
| TN buffer | 10 mM Tris HCl pH 8.0, 150 mM NaCl |
Table 1: Preparation of solutions.
| Gene name | Primer sequence |
| TNF-alpha Fw | 5’-TGCTTCACGCTCCATAAGACC-3’ |
| TNFalpha Rev | 5’-CAAGCCACCTGAAGAAAAGG-3’ |
| IL1-beta Fw | 5’-TGGACTTCGCAGCACAAAATG-3’ |
| IL1-beta Rev | 5’-CGTTCACTTCACGCTCTTGGATG-3’ |
| rpl8 Fw | 5’-CTCCGTCTTCAAAGCCCAT-3’ |
| rpl8 Rev | 5’-TCCTTCACGATCCCCTTGAT-3’ |
Table 2: Primers used for RT-qPCR.
