The results demonstrate that the protocol developed is a straightforward method, which permits the induction of a full thickness burn wound in mice. Burns are induced using a preheated brass template (Figure 1A-C). The burned area appears as a circular wound with a white eschar and a hyperemic zone. The size of the burn wound is slightly larger at 24 hours after the burn injury as a result of the well-described phenomenon known as the burn injury progression, which is possibly due to acute inflammation22. After excision, burn wounds are reconstructed using allogeneic skin graft (Figure 3). On day 7 after the burn injury, wounds become vascularized5, which is an indication of successful engraftment. Epidermal keratinocytes migrate from the adjacent recipient skin in the effort to close the wound and bridge the gap between the two edges of the wounds. Microscopic analysis of H and E stained section of wounds revealed that the length of the neo-epidermis becomes significantly longer on day 7 after burn injury compared to day 3 after burn injury (Figure 4B). Prior to performing a large study, it is highly recommended that researchers complete a pilot study, which enables the exploration of a novel intervention, assessment of feasibility, identification of modifications to the method to ensure reproducibility. Statistically significant effects are difficult to detect in smaller samples, whereas increasing the sample size is one way to boost the statistical power of a test. For example, to detect a statistically significant difference (p < 0.05) in the rate of wound re-epithelialization (Figure 4) between groups, the sample size should be between six and eight mice per group. All experiments should be repeated at least twice. As matrix producing cells, such as fibroblasts, migrate from the recipient tissue into the graft, key components of the extracellular matrix, including collagen I and fibronectin become highly expressed in the newly formed matrix (Figure 5).
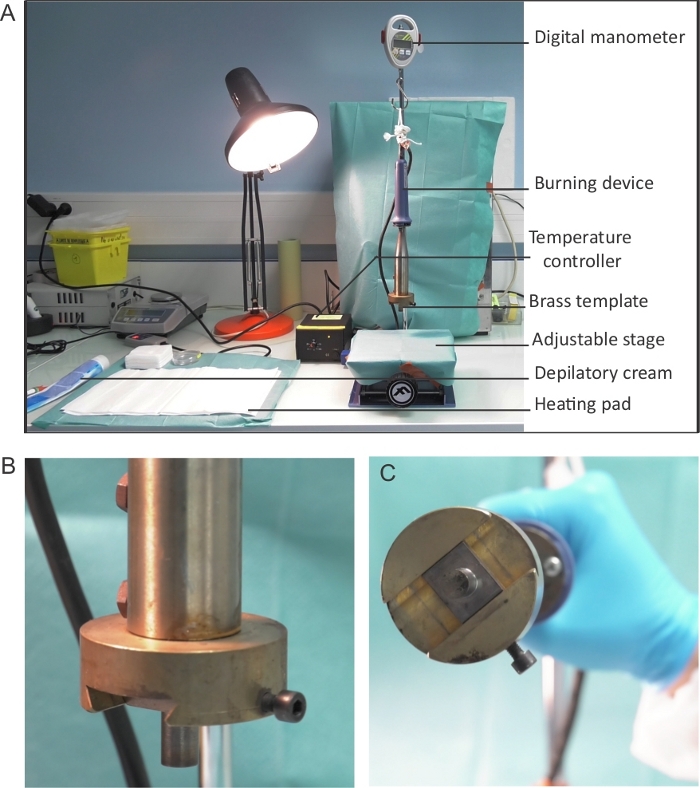
Figure 1: Burning device setup. (A) Placement and set-up of the burning device. The burning device is connected to the temperature controller and is attached to the digital monometer to enable the monitoring of pressure. The burning device is suspended above an adjustable stage – flat surface onto which mice are placed for the induction of burn. (B-C) A close up image of the brass template used to induce wound burns. (C) The diameter of the brass template is 1 cm. Please click here to view a larger version of this figure.
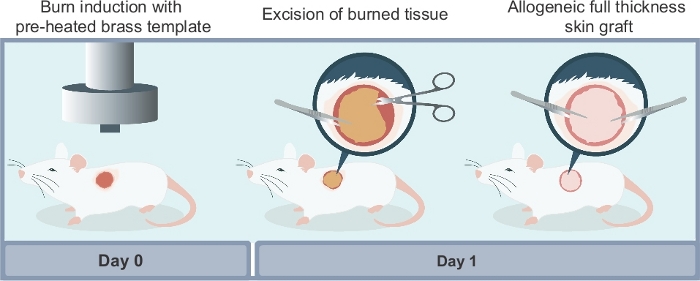
Figure 2: Schematic illustration of the different steps required to reproduce the experimental model described in this article. There are three main steps to the procedure: (i) induction of the burn wound using a preheated brass template; (ii) surgical excision of the non-viable necrotic tissue at 24 hours after the burn injury; (iii) surgical wound reconstruction using a full thickness allogeneic skin graft harvested from a donor mouse. Please click here to view a larger version of this figure.
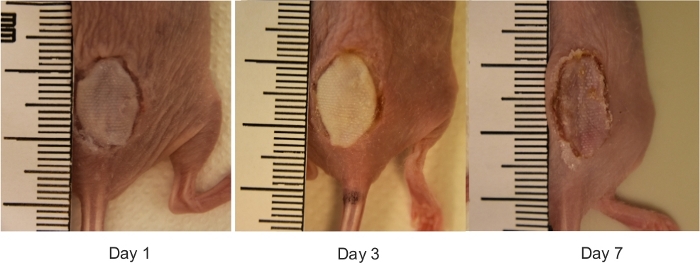
Figure 3: The macroscopic view of reconstructed mouse burn wounds. Representative digital images of burn wounds reconstructed with allogeneic skin grafts on days 0, 1, 3 and 7 after burn injury. The ruler on images is in millimeters. Please click here to view a larger version of this figure.
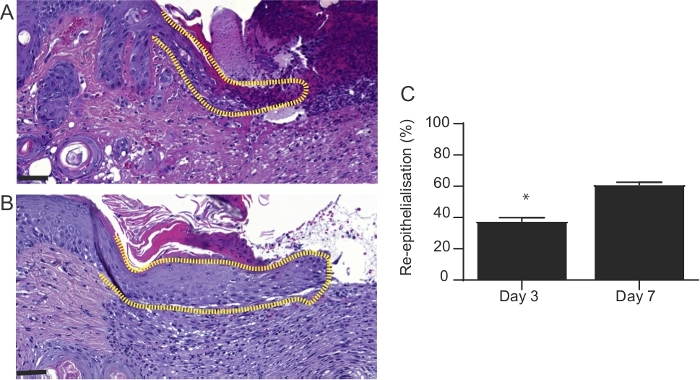
Figure 4: Microscopic appearance of wounds at 3 and 7 days after burn injury. H&E-stained sections of wounds 3 and 7 days after burn injury. The length of neo-epidermis (dotted line) is significantly increased in (A) day 3 wounds compared to (B) day 7 wounds. In (A) and (B), the scale bar is 100 µm. (C) Graphical representation of the percentage of wound re-epithelialization. This was evaluated by measuring the length of neo-epidermis at day 3 and 7 post-burn injury and expressed as a percentage of the whole wound length. Results represent mean ± S.E.M. (n = 6 mice in day 3 group; n = 6 mice in day 7 group, *p < 0.05; Student’s t-test). Please click here to view a larger version of this figure.
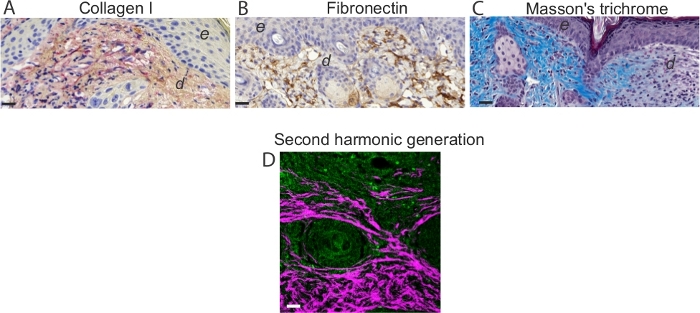
Figure 5: Assessment of the extracellular matrix and collagen I visualization. Representative images of immunohistochemistry analysis on day 7 mouse wounds stained for (A) collagen and (B) fibronectin. Note intense red staining in elongated spindle-shaped collagen I-positive cells. Note brown staining in fibronectin-positive cells in the dermis of day 7 wounds. Scale bar = 50 µm in all images. In (A) and (B), e denotes epidermis and d denotes dermis. (C) Visualization of collagen fibers and histological assessment of collagen deposition. (D) Representative TPEF/SHG collagen image of day 7 mouse wounds. Simultaneous TPEF/SHG acquisition using circular polarization and SHG signals were selectively processed to obtain a binary distribution of SHG after applying a threshold. TPEF images (green) and SHG images (white) were pseudo-colored and overlaid. Scale bar = 50 µm. Please click here to view a larger version of this figure.
