A 55-year-old woman presented with progressive visual deficits. Her medical history was unremarkable. On ophthalmological evaluation, bilateral reduction of visual acuity (6/10 in the right eye and 8/10 in the left eye) was revealed, and the computerized visual field showed complete bitemporal hemianopia. No further deficits were evident on neurological examination, but the patient reported persistent asthenia and an increase in hunger and thirst sensation in the previous 2-3 months, with a weight gain of 4-5 kg and frequent awakenings in the night for the need to urinate. On endocrinological evaluation, central hypercorticism and diabetes insipidus were revealed. The patient was treated with corticosteroids (hydrocortisone 30+15 mg/day and desmopressin 30+30 µg/day). On 24 h sleep-wake cycle and temperature monitoring, no significant alterations were noticed after the hormonal substitute therapy's optimization.
Brain MRI demonstrated a suprasellar tumor occupying the opto-chiasmatic cistern and invading the 3rd ventricle, with an irregular polycystic morphology, enhancing after gadolinium, suspected as the first hypothesis for a craniopharyngioma (Figure 1A-C). Advanced imaging analyses were performed, as illustrated in the current protocol. The tumor core segmentation highlighted the gadolinium uptake and corresponded to a volume of 7.92 cm3 (Figure 1D-E).
The visual pathways were the most critical to evaluate in the pre-surgical planning of this patient. The pyramidal tracts were also reconstructed to assess the microstructural correlate of the signal increase detected on the FLAIR T2-weighted image at the level of the right tract.
The optic pathway tractography reconstruction was investigated, particularly the optic chiasm dislocation in the presence of the tumor mass. The bilateral optic cranial nerves were also reconstructed. In the interface between the brain, bones, and blood vessels, susceptibility artifacts did not allow for full reconstruction of the fibers connecting the optic chiasm to the optic nerves (Figure 2).
The pyramidal tracts diffusivity profile was investigated with along-tract DTI map statistics. At the level of the right posterior limb of the internal capsule, a focal FLAIR T2-weighted hyperintensity was present, corresponding to a 5% increase of the right MD measure (5th-7th segments) compared to the left side (Figure 3).
By considering such relationships between tumor and neural structures, the endoscopic endonasal extended transplant/transtuberculum approach was chosen36. The tumor removal was performed with a microsurgical two-hands technique. Initially, the tumor was centrally debulked, also draining its cystic component (Figure 4). Afterward, it was possible to progressively detach the craniopharyngioma from the neural structures, adopting the arachnoid as a cleavage plane (Figure 5). At the end of the surgery, complete tumor removal with the hypothalamus's anatomical preservation was achieved (Figure 6). The repair of the osteo-dural defect was performed with abdominal fat and naso-septal flap (Figure 7).
The postoperative course was uneventful, and the patient was discharged after four days in the right clinical conditions. The tumor turned out to be an adamantinomatous craniopharyngioma (WHO grade 1) on histological examination.
The patient developed complete panhypopituitarism at follow-up and was under complete substitution therapy with hydrocortisone, desmopressin, and levothyroxine. Visual deficits wholly regressed, and no alterations on neurological examination, 24 h sleep-wake cycle, and temperature monitoring were detected. Three months of brain MRI demonstrated a complete tumor removal, with no remnant or recurrence. Therefore, no adjuvant treatment was advised, and the patient is followed up with yearly clinical and neuroradiological examinations (Figure 8).
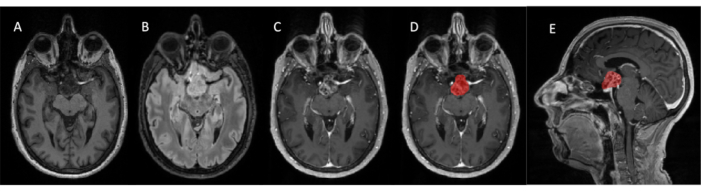
Figure 1. Preoperative anatomical MRI sequences (F/55 years). Axial view of T1-weighted (A) and FLAIR T2-weighted (B); axial (C, D) and sagittal (E) T1- after gadolinium administration (0.1 mm/kg). The tumor segmentation (red) overlaid to the gadolinium-enhanced T1-weighted image is shown in D and E. Please click here to view a larger version of this figure.
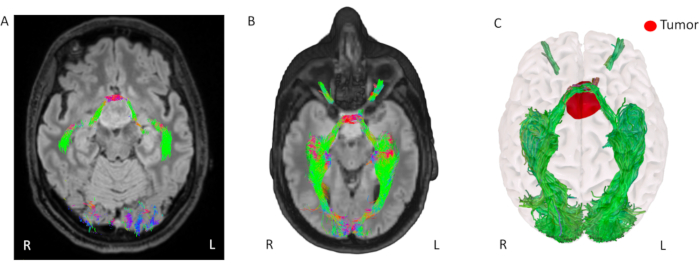
Figure 2. Preoperative 3D rendering of optic pathways tractography and tumor segmentation. (A) Axial slice of the FLAIR T2-weighted image overlays the optic chiasm tractography, localized anteriorly to the tumor. (B) 3D volume rendering of the FLAIR T2-weighted image, selecting an axial plane and overlaid the optic pathways tractography. (C) 3D volume rendering of the brain surface, optic pathways tractography, and tumor segmentation in red. All the panels' tractography streamlines are colored by the RGB directionality color map (red: lateral-lateral, green: anterior-posterior, and blue: inferior-superior). Please click here to view a larger version of this figure.
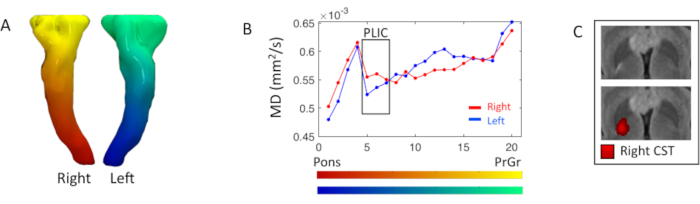
Figure 3. Pyramidal along-tract DTI measure analysis. (A) 3D rendering of the bilateral pyramidal tracts or corticospinal tract (CST), colored based on the Laplacian inferior-superior segmentation gradient. (B) Right (red) and left (blue) CST mean diffusivity (MD) profiles resulting from the partitioning of the tract into twenty segments displayed in the color maps in A; segments start at the level of the pons towards the precentral gyrus (PrCr). The black box highlights the segments at the posterior limb of the internal capsule (PLIC) (5th-7th). (C) Axial view of FLAIR T2-weighted image at the PLIC level, with and without the right CST connectivity map, where a brighter red intensity corresponds to a higher streamline density. Please click here to view a larger version of this figure.
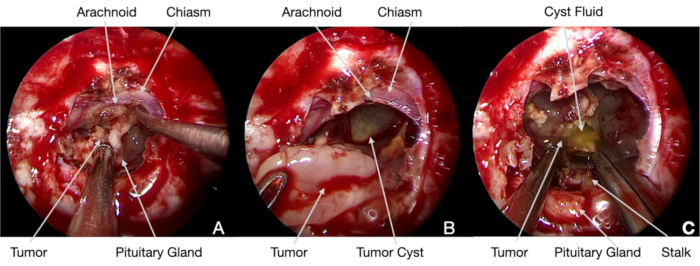
Figure 4. Intraoperative endoscopic images. (A) 0° scope, after dural opening, the tumor was initially detached by the chiasm, adopting the arachnoid as a cleavage plane. (B) and (C), afterward, it was centrally debulked, and the cyst was progressively drained. Please click here to view a larger version of this figure.
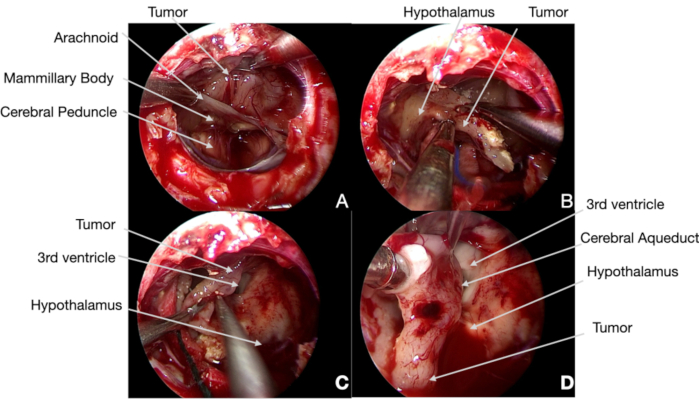
Figure 5. Intraoperative endoscopic images. (A) 0° scope, the craniopharyngioma is cleaved by the arachnoidal plane with the help of neuronavigation, showing the tumor and the neural structures (identified according to our current protocol). Therefore, the mammillary bodies can be spared to avoid permanent hypothalamic damages. (B) and (C) afterward, it was possible to resect the tumor by the medial hypothalamic surfaces, avoiding any tractions not to injure such neural structure. (D) During the removal of the tumor's intra-ventricular portion, particular care was paid in re-opening the cerebral aqueduct and Monro foramina to avoid postoperative acute hydrocephalus. Please click here to view a larger version of this figure.
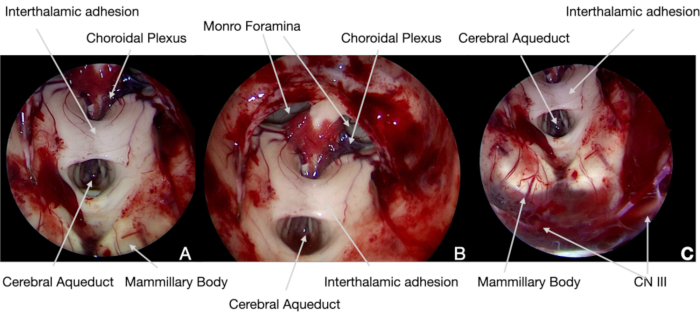
Figure 6. Intraoperative endoscopic images. (A) and (B) 30° scope, at the end of the surgery, the neural structure of the 3rd ventricle has been explored with angled optics to confirm the complete tumor removal and demonstrate its anatomical integrity. (C) At the bottom of the surgical field, it was possible to identify the CN III, under the Liliequist membrane: its function, as the MEPs, SEPs, and other CNs, had been continuously controlled with intraoperative neurophysiological monitoring. Please click here to view a larger version of this figure.
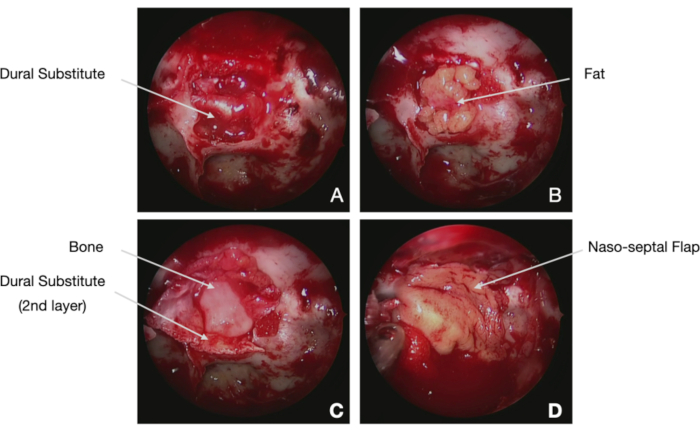
Figure 7. Intraoperative endoscopic images. (A) 0° scope, closure of osteo-dural defect requires a multilayer technique, adopting dural substitute, abdominal fat, eventually bone, and naso-septal flap. The first layer is constituted by intracranial intradural positioning of the first layer of a dural substitute. (B) The following step is represented by abdominal fat placement to fill the surgical cavity; particular care should be paid to avoid overpacking. (C) The second layer of dural substitute is adopted to cover the fat, and it can be maintained in position thanks to a rigid scaffold, as a piece of bone or cartilage (gasket seal technique). (D) Finally, the naso-septal flap or a free graft of septum or middle turbinate is used to cover the multilayer closure. Please click here to view a larger version of this figure.
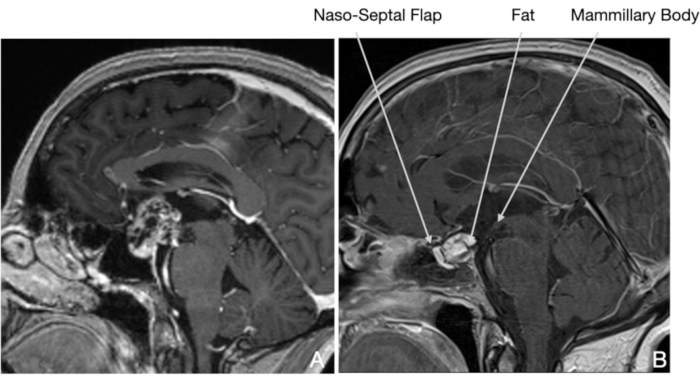
Figure 8. MRI, sagittal view T1-weighted after gadolinium administration (0.1 mm/kg). (A) Preoperative MRI demonstrates the tumor. (B) Post-operatively, the complete tumor removal with the mammillary bodies' anatomical preservation and the hypothalamic structures are visible. Please click here to view a larger version of this figure.
