The Institutional Review Board (IRB) of SUNY Upstate Medical University approved this protocol.
1. Participant screening
- Perform all research methods with IRB approval by the Declaration of Helsinki.
- Recruit non-disabled adults who do not have any neurological or musculoskeletal issues that prevent upper extremity motor task performance.
- Recruit chronic stroke survivors whose stroke onset is at least six months before study participation and who have mild-to-moderate upper extremity motor impairment, indicated by Fugl-Meyer Assessment of upper extremity score of 19 to 60 out of 66, and can extend hemiparetic wrist and fingers at least 10 degrees voluntarily.
- Schedule potential participants to attend a data collection session.
- Obtain written informed consent from all research participants before initiating any experimental procedures.
- Screen all participants for study participation eligibility using questionnaires regarding their demographics, previous arm injury history, hand dominance, and confidence in specific fine hand motor skill tasks.
2. Upper Extremity Motor Outcome Measures
- Perform the Perdue Pegboard Test with the standard procedure10.
- Perform the Fugl-Meyer Assessment of Upper Extremity Motor (FMA-UE) using the standard procedure11,12.
3. Psychosocial and cognitive-behavioral assessments
- Have participants complete the following questionnaires using the online survey platform: Edinburg Handedness Inventory; a questionnaire for previous experience on the use of chopsticks.; and a self-efficacy questionnaire for the use of chopsticks.
4. Preparation of Goal-directed Arm Reaching Tasks
- Prepare the motion capture camera system for kinematic recording.
- Calibrate the motion capture camera using the motion capture workstation software.
- Set the origin of the world coordinate using the motion capture workstation software.
- Place all marker triads on a table in the field of view of motion capture cameras and check if all marker triads are within the field of view.
- Prepare the motion capture data acquisition software to build the skeletal model.
- Import the marker sets from the motion capture workstation software to the motion capture data acquisition software.
- Activate virtual sensors (i.e., marker triads).
- Set world axes.
- Assign virtual sensors to body segments of the skeleton model.
- Set up goal-directed arm reaching task conditions.
- Place a table at the center of the motion capture cameras field of view.
- Put the laminated goal-directed arm reaching template paper at the designated area on the table.
- Prepare a pair of chopsticks on the table.
- Prepare to play the auditory cue audio file.
- Prepare the task instruction scripts.
- Test the motion capture system to ensure it is working appropriately.
- Set up the participant.
- Attach the reflective marker triads to the skin of the participant's arms, hands, and trunk. Use the following description for the marker triad locations:
A marker triad for the trunk: between medial borders of the scapulae
A marker triad for each upper arm: in the middle of the lateral surface of the upper arm
A marker triad for each forearm: in the middle of the dorsal surface of the forearm
A marker triad for each hand: in the middle of the dorsal surface of the 3rd metacarpal bone - Prepare a chopstick with a marker triad.
- Place a marker triad on a table located center of the field of view of motion capture cameras.
- Digitize the participant's body segments using an upper extremity joints and trunk skeleton model that includes following landmarks using the motion capture data acquisition software:
Upper trunk: a spot between C7 and T1 vertebrae
Lower trunk: a spot between T12 and L1 vertebrae
Shoulder (glenohumeral joint), two spots equidistance from center of the head of humerus
Elbow: two spots on the medial and lateral elbow that are equidistant from the joint center
Wrist: two spots on the medial and lateral wrist that are equidistant from the joint center
Hand: the tip of the third phalanx of each hand - Digitize the tip of the chopstick with a marker triad using the motion capture data acquisition software.
- Digitize the home position and target position using the marker triad located on the table using the motion capture data acquisition software.
- Attach the reflective marker triads to the skin of the participant's arms, hands, and trunk. Use the following description for the marker triad locations:
5. Performance of Goal-directed Arm Reaching Tasks
- Position the participant in a sitting position.
- Ask the participant to reach forward without trunk movement, then locate the table to position the target at approximately 80% of the participant's maximum arm reaching distance.
- Instruct the participant to maintain the upright trunk posture at the beginning of each task performance. There will be no restriction to the trunk movements during the task performance.
- Instruct the participant how to use chopsticks using a Youtube video (https://youtu.be/2Bns2m5Bg4M) to standardize the way to use the chopsticks.
- Perform the task condition 1 – Reaching and Pointing to a large target.
- Instruct the participant to hold a chopstick with the dominant hand (non-disabled adults) or the paretic hand (stroke participants). The participant will place the tip of a chopstick touching at the center of the home position. Instruct the participant to maintain the upright trunk posture at the beginning.
- Fixate the task condition template paper at the designated area on the table. The template paper includes two squares with a cross at the center of each square: one for the home position and the other one for the target area. For this task, the target square size is 1 x 1 cm2. The target position is located 20 in front of the home position.
- Describe the task instructions.
- State the following: "The goal of this task is to reach and tap the target area with the chopstick's tip as quickly and accurately as possible. You will hold a chopstick with your right (or left) [indicate the performing hand]. Place the chopstick's tip on the home position [indicate the home position]. When you hear a 'GO' signal, reach and tap the target [indicate the target] with the chopstick's tip as quickly as possible. Try to tap the center of the target as much as you can. You will have three seconds to tap the target. I will give you a 'STOP' signal 3 seconds after the 'GO' signal. If you did not tap the target within 3 seconds, bring the chopstick's tip to the home position and wait for the next trial. You will perform ten trials with a 10-second break between trials. Do you have any questions? [Address any questions that the participant has, then proceed to familiarization trial] You will have three trials as a practice. [After the practice trials, proceed to the actual trials] Now, we will perform actual trials. Try to reach and tap as quickly as you can."
- Play the auditory cue signal audio file with a computer to familiarize the participant with the cue.
- Perform three familiarization trials.
- Instruct the participant to be ready for the task performance. Ensure the participant fully understands the task performance procedure.
- Start motion capture recording with the motion capture data acquisition software.
- Play the auditory cue audio file with a computer.
- Perform 10 trials.
- Stop motion capture recording.
- Take a 2-minute break.
- Perform the task condition 2 – Reaching and Pointing to a small target.
- Instruct the participant to hold a chopstick with the dominant hand (non-disabled adults) or the paretic hand (stroke participants). The participant will place the tip of a chopstick touching at the center of the home position. Ask the participant to maintain the upright trunk posture at the beginning.
- Fixate the task condition template paper at the designated area on the table. For this task, the target square size is 0.3 X 0.3 cm2. The target position is located 20 in front of the home position.
- Describe the task instruction.
- State the following: "The goal of this task is the same as the previous task: reach and tap with the chopstick's tip the target as quickly and accurately as you can. We will use a smaller target [indicate the target]. The instruction is the same as the previous task. When you hear a 'GO' signal, reach and tap the target [indicate the target] with the chopstick's tip as quickly as possible. Try to tap the center of the target as much as you can. Do you have any questions? [Address any questions that the participant has, then proceed to familiarization trial] You will have three trials as a practice. [After the familiarization trials, proceed to the actual trials] Now, we will perform actual trials. Try to reach and tap as quickly as you can."
- Play the auditory cue signal audio file with a computer to familiarize the participant with the cue.
- Perform three familiarization trials.
- Instruct participant to be ready for the task performance. Ensure the participant fully understands the task performance procedure.
- Start motion capture recording with the motion capture data acquisition software.
- Play the auditory cue audio file with a computer.
- Perform 10 trials.
- Stop motion capture recording.
- Take a 2-minute break.
- Perform the task condition 3 – Reaching and Picking up a large target object.
- Instruct the participant to hold a pair of chopsticks with the dominant hand (non-disabled adults) or the paretic hand (stroke participants). The participant will place the tips of chopsticks touching at the center of the home position. Ask the participant to maintain upright trunk posture at the beginning.
- Fixate the task condition template paper at the designated area on the table. For this task, the target object is a plastic cube 1 cm on edge. The target object is located 20 in front of the home position.
- Place the target object on the target area.
- Describe the task instructions.
- State the following: "The goal of this task is to reach and pick up a plastic cube [indicate the cube] with a pair of chopsticks as quickly as possible, about an inch in height without dropping. You will hold a pair of chopsticks with your right (or left) [indicate the performing hand]. Place the chopsticks' tips on the home position [indicate the home position]. When you hear a 'GO' signal, reach and pick up the cube [indicate the target] with the chopsticks as quickly as you can, about an inch in height. You will have three seconds to pick up the target. I will give you a 'STOP' signal 3 seconds after the 'GO' signal. If you did not pick up the target within 3 seconds, bring the chopsticks' tips to the home position and wait for the next trial. You will perform ten trials with a 10-second break between trials. Do you have any questions? [Address any questions that the participant has, then proceed to familiarization trial] You will have three trials as a practice. [After the familiarization trials, proceed to the actual trials] Now, we will perform actual trials. Try to reach and pick up as quickly as you can."
- Play the auditory cue signal audio file with a computer to familiarize the participant with the cue.
- Perform three familiarization trials.
- Instruct participant to be ready for the task performance. Ensure the participant fully understands the task performance procedure.
- Start motion capture recording with the motion capture data acquisition software.
- Play the auditory cue audio file with a computer.
- Perform 10 trials.
- Stop motion capture recording.
- Take a 2-minute break.
- Perform the task condition 4 – Reaching and Picking up a small target object.
- Instruct the participant to hold a pair of chopsticks with the dominant hand (non-disabled adults) or the paretic hand (stroke participants). The participant will place the tips of chopsticks touching at the center of the home position. Ask the participant to maintain upright trunk posture at the beginning.
- Fixate the task condition template paper at the designated area on the table. For this task, the target object is a plastic cube 0.3 cm on edge. The target object is located 20 in front of the home position.
- Place the target object on the target area.
- Describe the task instructions.
- State the following: "The goal of this task is the same as the previous task: reach and pick up a plastic cube with a pair of chopsticks as quickly as you can. We will use a smaller plastic cube [indicate the target]. The instruction is the same as the previous task. When you hear a 'GO' signal, reach and pick up the cube [indicate the target] with chopsticks as quickly as possible. Do you have any questions? [Address any questions that the participant has, then proceed to familiarization trial] You will have three trials as a practice. [After the familiarization trials, proceed to the actual trials] Now, we will perform actual trials. Try to reach and tap as quickly as you can."
- Play the auditory cue signal audio file with a computer to familiarize the participant with the cue.
- Perform three familiarization trials.
- Ask participant to be ready for the task performance. Make sure the participant fully understands the task performance procedure.
- Start motion capture recording with the motion capture data acquisition software.
- Play the auditory cue audio file with a computer.
- Perform the actual 10 trials.
- Stop motion capture recording.
- Take a 2-minute break.
- Perform the Intrinsic motivation inventory (IMI) for the use of chopsticks using online survey platform.
6. Kinematic data analysis
- Export the data of the following landmarks from the motion capture data acquisition software. Export position data in the x-, y-, and z-axes as a text file for each task condition.
Tip of a chopstick
Home position on the table
Target position on the table
Hands
Elbow joints
Shoulder joints (glenohumeral joints)
Trunk (at C7) - Preprocess the kinematic data.
- Use custom programming script to process the kinematic data.
- Filter and smooth the raw position data using a 3rd order Butterworth low pass filter with a 3 Hz cutoff.
- Calculate the resultant of x-, y-, and z-direction position of the performing hand.
- Determine movement onset and offset of each goal-directed arm reach.
- To determine the reaching movement onset and offset, use the tangential velocity (the first derivative of the position data) from the resultant of the 3-dimensional position of the performing hand.
- Define movement onset as the first frame of the reach, where the tangential velocity is above 0.01 m/s.
- Define movement offset as the last frame of the reach, where the tangential velocity is above 0.01 m/s.
- Inspect the individual reaching movement onset and offset visually to ensure the onset and offset are correctly labeled.
- Determine the peak velocity. The peak velocity is defined as the maximum tangential velocity amplitude of the trial that exceeds the amplitude of 0.2 m/s, and the time interval between 2 peaks must be at least 2 seconds13.
- Calculate kinematic variables of reaching movements.
- Calculate movement duration (MD). Calculate the time difference between movement onset and offset13.
- Calculate peak velocity (PV). Calculate the highest velocity during each of the reaches.
- Calculate absolute and relative time to peak velocity (TTPV and TTPV % of movement duration)13.
- Calculate the time difference between movement onset and peak velocity (absolute TTPV).
- Calculate the percentage of TTPV relative to movement duration (relative TTPV).
- Calculate log dimensionless jerk.
- Calculate the third derivative from the resultant of the 3-dimensional position of the performing hand, then calculate the log dimensionless jerk of each arm reaching movement.
- Calculate trunk displacement during goal-directed arm reaching movement9,14.
- Calculate the trunk displacement.
- Calculate the distance difference of the trunk landmark between movement onset and offset. Use the following equation.

Where X, Y, and Z are the trunk landmark positions in x-, y-, and z-axis, respectively; 1 is the time frame at the reaching movement onset; k is the time frame at the reaching movement offset.
- Calculate the distance difference of the trunk landmark between movement onset and offset. Use the following equation.
- Calculate shoulder trajectory length.
- Calculate the shoulder landmark's travel distance between arm reaching movement onset and offset. The shoulder landmark is a virtual landmark digitized from the motion capture data acquisition software using the upper extremity skeleton model. Use the following equation for the shoulder trajectory length calculation.

Where X, Y,and Z are the positions of the shoulder landmark in x-, y-, and z-axis, respectively; t is the time frame; t=1 is the time frame at the reaching movement onset; t=k is the time frame at the reaching movement offset
- Calculate the shoulder landmark's travel distance between arm reaching movement onset and offset. The shoulder landmark is a virtual landmark digitized from the motion capture data acquisition software using the upper extremity skeleton model. Use the following equation for the shoulder trajectory length calculation.
- Calculate the trunk displacement.
These results are preliminary data from two non-disabled young adults and two chronic stroke survivors with mild motor impairment (Fugl-Meyer Scores of these two participants were above 60 out of 66). Non-disabled participants were right-handed and performed the tasks with their right hand. Stroke participants were also right-handed before the stroke and both had right hemiparesis. They also performed the task with their right hand. These kinematic variables between populations and between target conditions were compared using the Wilcoxon signed-rank test.
Shoulder trajectory length is a more sensitive measure of trunk compensation during goal-directed arm reaches (Figure 1).The trunk displacement and shoulder trajectory length were compared to determine which variable would be more appropriate to represent trunk compensation during goal-directed arm reaches. There was no significant difference in trunk displacement between non-disabled adults and chronic stroke survivors in all four task conditions. However, there was a significantly greater shoulder trajectory length for chronic stroke survivors than non-disabled adults for reaching and picking up tasks.
Chronic stroke survivors had different kinematic characteristics of goal-directed arm reaches than non-disabled young adults across different task conditions (Figure 2). Chronic stroke survivors showed significantly slower (Figure 2A & B), more feedback-dependent (Figure 2C), and jerkier (Figure 2D) goal-directed arm reaches across four different task conditions compared to non-disabled adults. Further, chronic stroke survivors demonstrated significantly more trunk compensation than non-disabled adults during goal-directed arm reaches (Figure 2E).
Task complexity impacted kinematic variables of goal-directed arm reaching movement (Figure 2 & 3). Both non-disabled adults and chronic stroke survivors demonstrated slower, feedback-dependent, and jerkier goal-directed arm reaches for the more complex task requiring greater hand dexterity than the simple pointing task (Figure 2). There was no difference in shoulder trajectory length between two populations for the pointing tasks, while stroke survivors showed significantly greater shoulder trajectory length than non-disabled young adults for the picking up tasks (Figure 2). Further, motor performance had more variability across trials for the more complex task compared to the simper task (Figure 3).
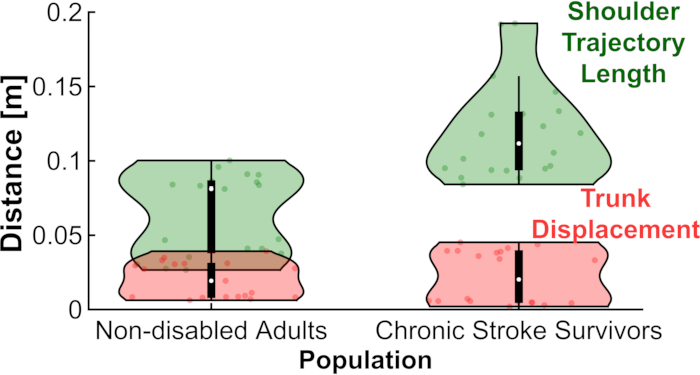
Figure 1. Comparison of two different kinematic measures of trunk compensation during goal-directed arm reaches. Green violin plots indicate the Shoulder Trajectory Length, and red violin plots show the Trunk Displacement. Please click here to view a larger version of this figure.
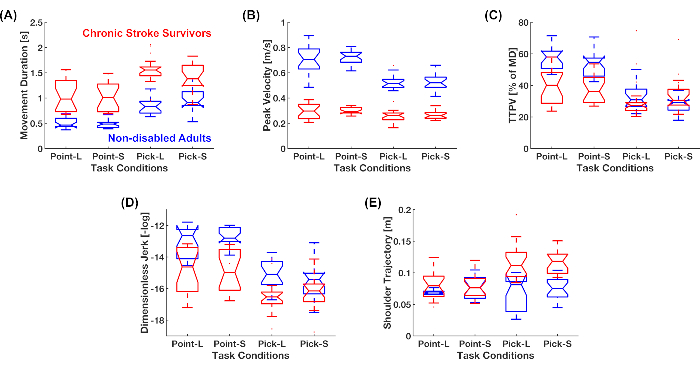
Figure 2. Comparison of goal-directed arm reaching kinematics in different task conditions between non-disabled adults and chronic stroke survivors. (A) Movement duration. Red boxplots are data of chronic stroke participants, and blue boxplots are data of non-disabled adults. (B) Peak velocity amplitude. (C) Relative time to peak velocity. This variable is the time to peak velocity as a percentage of movement duration. (D) Log dimensionless jerk. This variable indicates the movement's smoothness. A higher negative value in this variable means a jerkier movement. (E) Shoulder trajectory length. This variable indicates the amount of trunk compensation during goal-directed arm reaches in all x-, y-, and z-directions. Please click here to view a larger version of this figure.
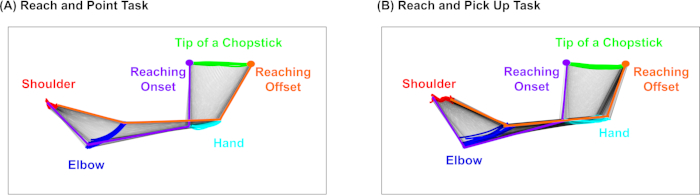
Figure 3. Visualization of goal-directed arm reaching kinematics. (A) Goal-directed arm reaching performance of reach and point task with a large target. (B) Goal-directed arm reaching performance of reach and pick up task with a large object. Positions of shoulder, elbow, hand and tip of a chopstick landmarks are visualized with colored dots for all ten arm reaching trials for the task condition. Positions of those landmarks, arm, and hand at the movement onset and offset are highlighted in purple and orange, respectively. Please click here to view a larger version of this figure.
