Interpretation of the ACh-test and rechallenge are based on criteria defined by the COVADIS study group4. A positive diagnosis for CAS is defined as (i) reproduction of the previously reported symptoms such as chest pain, shortness of breath, or other symptoms and (ii) the induction of ischemic ECG changes (ST-segment elevation or depression, or U-waves) in reaction to ACh. (Figure 2). It is therefore important to register a 12-lead-ECG continuously throughout the test and monitor for ischemic changes during ACh administration or when symptoms are reported. Finally, the distinction between epicardial and microvascular spasm is made by comparing coronary diameter reduction in reaction to the spasm provocating dose and NTG (Figure 2 and Figure 4). When epicardial vasoconstriction of >90% is evident on angiography, epicardial spasm can be diagnosed, and when this is <90% occurs, this is considered to be a microvascular spasm. Furthermore, the epicardial spasm may occur within the confines of one isolated coronary segment (focal spasm) or in ≥2 adjacent coronary segments (diffuse spasm)4.
When performing an ACh rechallenge, it can be useful to obtain a VAS score at the initial spasm provocation and rechallenge to quantify the improvement in symptoms. Improvement in provoked ischemic ECG changes, changes in APV, and severity of vasoconstriction on angiography can help as an objective measure of the preventive effect of NTG (Figure 2, Figure 3, and Figure 4).
Continuous assessment of Doppler flow provides valuable information during spasm provocation. Most importantly, it provides a safety feature as flow alterations most often occur prior to ECG changes (Figure 5). This improves operator awareness and patient safety.
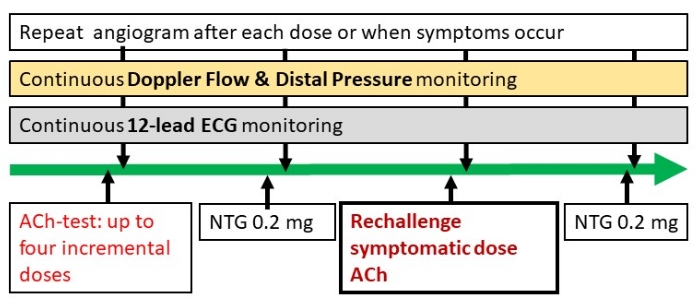
Figure 1: Flow chart protocol. The ACh rechallenge can be applied to any protocol version and can therefore be performed according to local protocol. After NTG administration, the spasm provocative dose can be readministered to perform the rechallenge. Please click here to view a larger version of this figure.
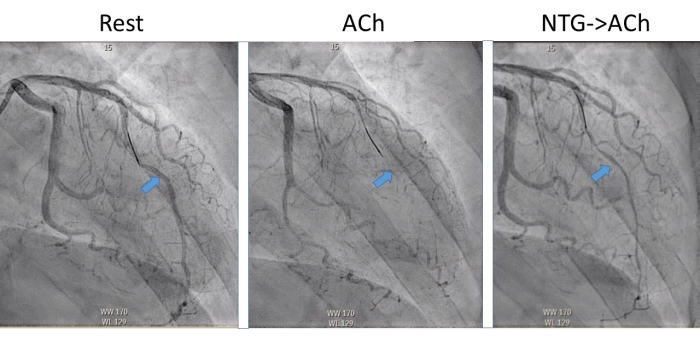
Figure 2: Coronary angiographical evaluation of the NTG rechallenge. The coronary angiography performed during rest shows that no significant lumen reduction is present in the LAD depicted by the arrow (Rest). At the fourth dose (ACh) <90%, epicardial lumen reduction occurs together with ECG changes and recognizable symptoms and therefore meets the diagnostic criteria for epicardial vasospasm. The last image depicts the preventive effect of NTG when the coronary artery is rechallenged after intracoronary administration of NTG. Now some vasoconstriction occurs although no >90% lumen reduction and the severity of anginal complaints are reduced. Please click here to view a larger version of this figure.
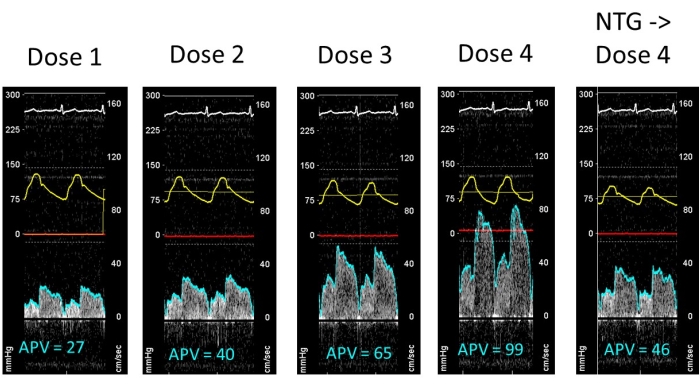
Figure 3: Example of APV changes during spasm provocation. At the fourth dose, epicardial vasoconstriction causes very high APV values, whereas the preventive effect of NTG causes lower APV values because the epicardial coronary artery does not constrict. Please click here to view a larger version of this figure.
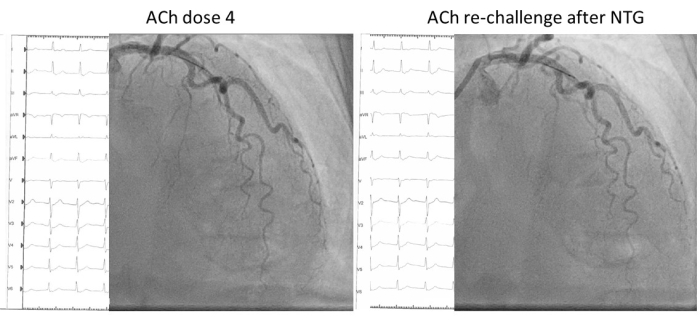
Figure 4: Example of a non-responder. In this example, the patient experiences recognizable anginal symptoms and ischemic ECG changes at the fourth acetylcholine dose without epicardial vasospasm consistent with the diagnosis of microvascular spasm according to COVADIS (left). After nitroglycerine administration, when symptoms have disappeared and ECG changes have normalized, the rechallenge with the same ACh dose commenced. Besides some epicardial vasodilation, the patient experienced symptoms and ischemic ECG changes of comparable severity compared to the spasm provocative dose. Please click here to view a larger version of this figure.
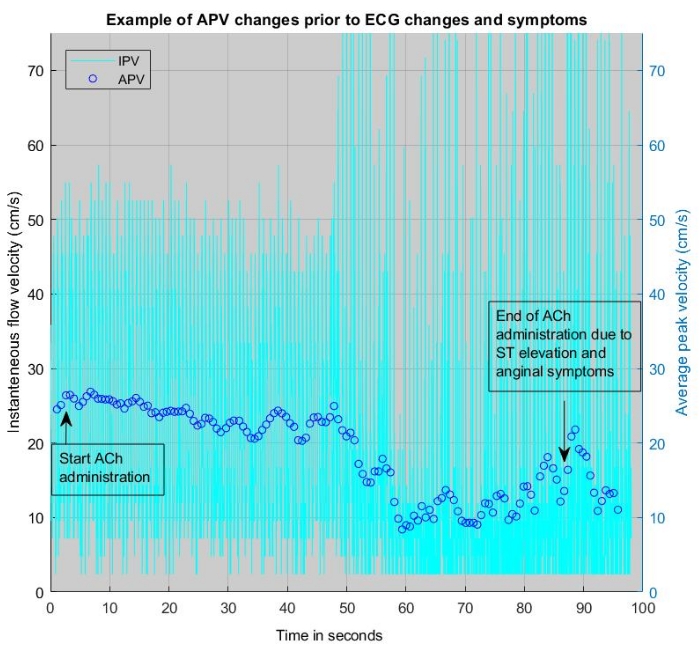
Figure 5: Example of APV changes during ACh infusion where a change in APV precedes symptoms or ECG changes and can be heard as a change in pitch of the acoustic signal. This example is from a 3 min infusion with acetylcholine. Please click here to view a larger version of this figure.
Supplementary Material: Instruction for preparing the syringes for ACh spasm provocation. Please click here to download this File.
