The model described here is a photothrombotic stroke model by Rose Bengal injection and intact skull illumination for 20 min, at a constant 561 nm wavelength and 25 mW output power at the fiber. Although the complete photothrombotic surgery lasts 30 min, the animal is kept under low anesthesia and the brain damage is moderate. Approximately 10 min after transfer to their cages, all the animals were awake, freely moving in the cage, and interacting with littermates.
Infarct volumetry was performed using cresyl violet stained serial coronal brain sections 24 h after stroke induction (Figure 2A). The mean infarct volume was 29.3 mm3, representing 23% of one brain hemisphere. Moreover, the variability of this stroke model is exceptionally low with a standard deviation of approximately 3.5% (Figure 2B). The lesion area encompasses the motor cortex without the affection of subcortical structures.
Photothrombosis caused a moderate, long-term sensorimotor impairment, indicated by the composite Neuroscore17 (Figure 3); general and focal deficits were measured 24 h, 3 days and 7 days after surgery. The general Neuroscore has five items, including the evaluation of the fur, ears, eyes, posture, and spontaneous activity, with a maximum score of 18 (Table 1). The focal Neuroscore comprises seven items, including the evaluation of body symmetry, gait, climbing, circling behavior, forelimb symmetry, compulsory cycling, and whiskers response, with a maximum score of 28 (Table 2). Stroke animals had a significant change in the composite neuroscore 24 h after surgery compared to Sham-operated animals. These differences persisted, although stroke mice improved over time (Figure 3).
Mortality during the observation time rarely occurs in 1-2% of the animals. In this report, none of the 10 animals studied had to be excluded and all of them survived the 7-day observation period. The body weight and temperature changes in the mice were monitored at 24 h, 3 days, and 7 days after surgery (Figure 4A,B). Data showed that body weight and temperature were decreased 24 h after surgery only in the Rose Bengal + illumination group, but recovered to the level of the Sham-operated animals in 3 days after surgery.
To confirm an induction of ischemic changes, 24 h after surgery, the animals underwent a laser imaging test. A laser speckle contrast imaging measured blood perfusion of the cortex for a duration of 1 min and an averaged color-coded picture was obtained for each animal. This demonstrates that Rose Bengal or laser illumination alone does not produce a lesion, while simultaneous application of Rose Bengal and laser illumination generates a round hypoperfused area of 4 mm diameter surrounded by a narrow oligemic zone (Figure 5A). In addition, a cresyl violet and Tunel staining for assessment of the infarct volume 24 h after surgery revealed no tissue damage either in Rose Bengal or laser illumination surgeries. On the other hand, Rose Bengal + laser illumination generated a well-demarcated lesion (Figure 5B).
Table 1: General Neuroscore. For each of the five general deficits measured, animals can receive between 0 and 4 points depending on the severity. The scores on the five areas are then summed to provide a total general score ranging from 0-18. Please click here to download this Table.
Table 2: Focal Neuroscore. For each of the seven general deficits measured, animals can receive between 0 and 4 points depending on the severity. The scores on the five areas are then summed to provide a total general score ranging from 0-28. Please click here to download this Table.
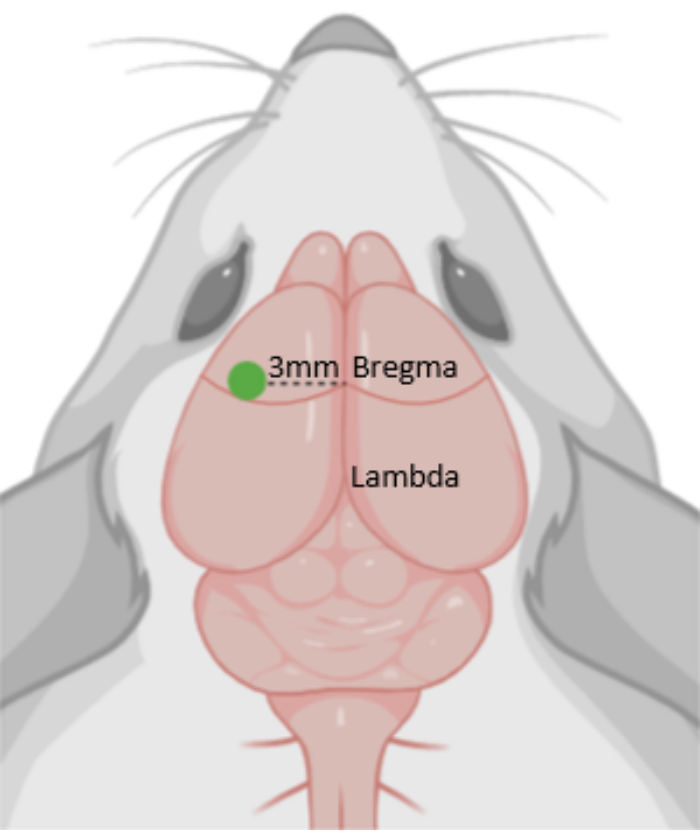
Figure 1: Photothrombosis (PT). Diagram depicting the photothrombotic area, 3 mm from Bregma. The green dot indicates the position of the laser. Please click here to view a larger version of this figure.
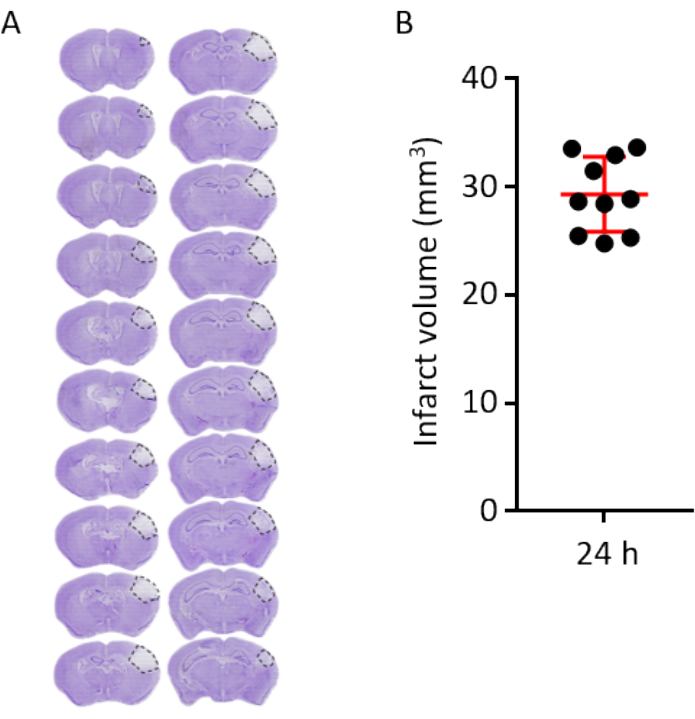
Figure 2: Volumetric infarct analysis and infarct outcome 24 h after PT. (A) Representative cresyl violet stained coronal brain, sections every 120 µm at 24 h after PT. Dashed lines demarcate the lesion area. (B) Infarct volume analysis of 10 brains (each dot representing one individual brain) 24 h after PT. The horizontal red line represents the mean (29.32 mm3), error bars indicate standard deviation (3.45 mm3). Please click here to view a larger version of this figure.
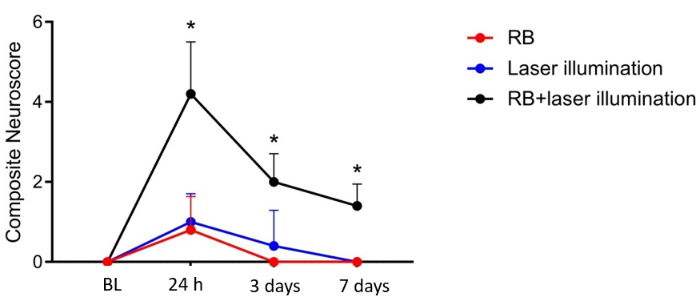
Figure 3: Neuroscore for functional deficits after PT. Composite Neuroscore before, 24 h, 3 days, and 7 days after PT. BL = before PT, RB = Rose Bengal. n = 5 per group. *p < 0.05. Please click here to view a larger version of this figure.
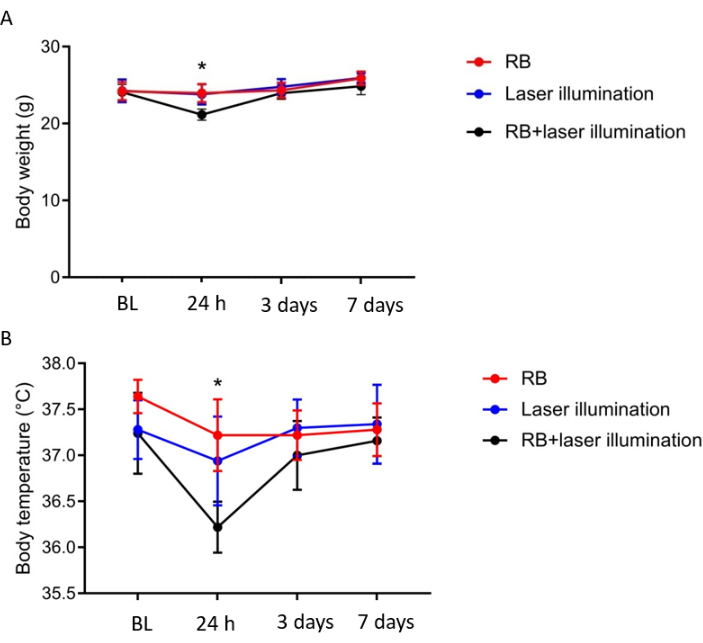
Figure 4: Body weight and temperature analysis after PT. (A) Body weight and (B) temperature was slightly reduced in PT animals compared to Sham-operated groups at 24 h and recovered 3 days after PT. BL = before PT, RB = Rose Bengal. n = 5 per group.*p < 0.05. Please click here to view a larger version of this figure.
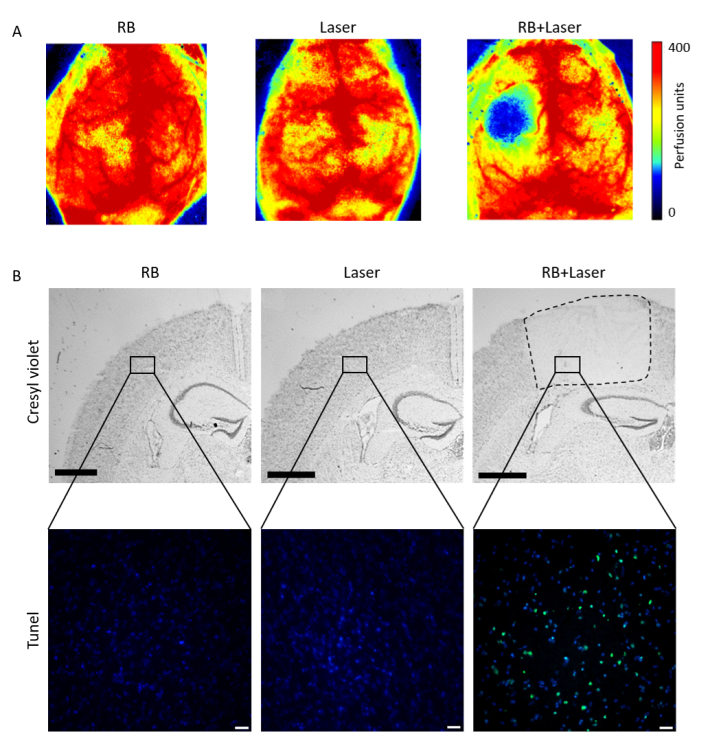
Figure 5: Lesion confirmation after PT. (A) Laser Speckle imaging (B) Cresyl violet (upper panels) and Tunel staining (lower panels) confirmed the lesion only after administration of Rose Bengal and subsequent laser illumination. RB = Rose Bengal. Scale bar = 1,000 µm in upper panel B, scale bar = 20 µm in lower panel B. Please click here to view a larger version of this figure.
