The tensometric small chamber myography protocol explained here is the standard method for measuring vascular reactivity in small and large arteries and allows for simultaneous measurements of vascular reactivity in up to four blood vessel segments from the same experimental small laboratory animal. In this report, we specifically use the system to measure endothelial function in the isolated mouse aorta (Figure 1). In this protocol, isolated aortic segments are mounted onto a small organ chamber (Figure 2) between two small stainless steel pins (Figure 3). The myograph chamber can hold up to 8 mL of buffer solution and provide a semi-physiologic environment for the isolated vessels for the duration of the experiments. It is very important that, prior to each experiment, the viability of each isolated segment is tested and verified. The standard protocol to establish the integrity and viability of each isolated vessel segment is to challenge the tissue with a high concentration of potassium chloride to induce smooth muscle membrane depolarization. In the scenario that the isolated vessel is healthy and responsive, we would be able to record the contractile force generation on the display (Figure 4). The peak of the recorded force is later used to normalize the force generation for the same segment in response to the agonists used during the protocol (e.g., phenylephrine). In order to measure endothelium-mediated vasorelaxation, it is necessary to pre-contract the aortic tissue with the sub-maximum concentration (10 µM) of phenylephrine, which causes smooth muscle-mediated contraction and force generation (Figure 5). When the phenylephrine-induced contraction reaches a plateau (Figure 6), increasing doses of acetylcholine are applied in multiple steps to achieve the maximum vasorelaxation in the isolated segment (Figure 6). The level of vessel relaxation is an indirect measurement of endothelium-mediated nitric oxide production. To further confirm that acetylcholine-induced vasorelaxation in aortic rings is due to the production of nitric oxide, aortic segments are pre-treated with a general inhibitor of nitric oxide production (200 µM of L-NAME) for 30 min prior to phenylephrine application. As shown in Figure 7, L-NAME is able to completely block acetylcholine-induced vasorelaxation in the pre-contracted aorta, highlighting the fact that acetylcholine induces aortic vasorelaxation through increasing nitric oxide production. On the other hand, the removal of the endothelial layer from the aortic segments also blocks acetylcholine-induced vasorelaxation, underscoring the role that the endothelium plays in blood vessel relaxation (Figure 8).
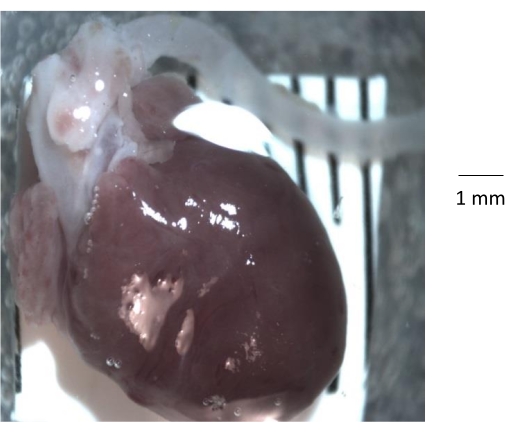
Figure 1: Gross anatomic view of the heart, aortic root, and descending aorta isolated from a 6-month-old control mouse. After removing the rib cage from the mouse, the heart and aorta are isolated from the rib cage and transferred to a clean silicone elastomer-coated Petri dish. Prior to isolating the aorta, it is important to remove all the fat and connective tissue and any blood clot from the lumen of the aorta. Please click here to view a larger version of this figure.
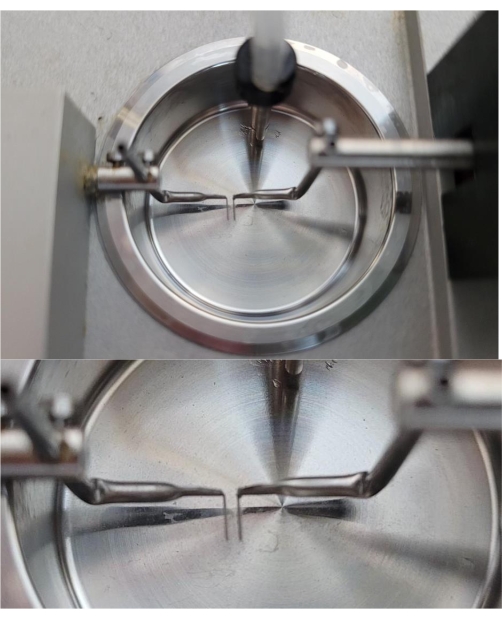
Figure 2: A representative image of a chamber of the myograph unit showing the 200 µm mounting pins. As shown, the two pins inside the myograph chamber are barely touching. Prior to using the chamber, it is critical to make sure that the pins are properly aligned. Please click here to view a larger version of this figure.
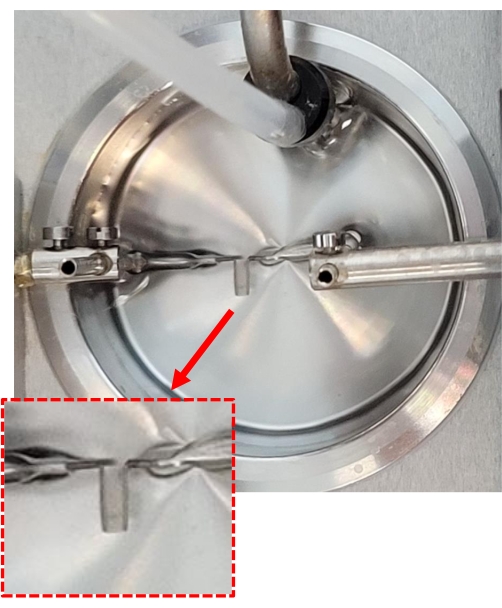
Figure 3: Anchoring the aortic segments onto the myograph chamber. A 2 mm mouse aortic segment isolated from a 6-month-old C57BL/6 mouse is held by two pins inside a myograph chamber. This is achieved by gently sliding the aorta onto the two mounting pins using forceps. The red dotted box shows the zoomed-in image of the 2 mm aortic segment that is mounted between two pins inside the myograph chamber. Please click here to view a larger version of this figure.
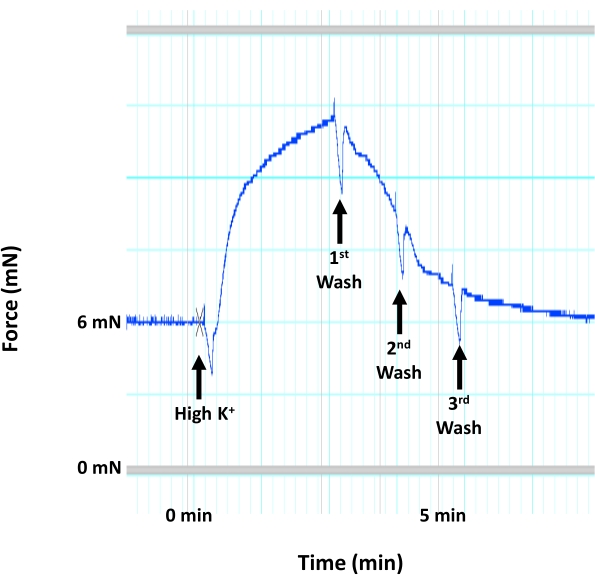
Figure 4: Aortic contraction due to smooth muscle membrane depolarization. Representative image showing the trace for mouse aortic contraction (force generation) in response to a high concentration of K+ (60 mM KCl) that would induce smooth muscle membrane depolarization and contraction within the medial layer of the aorta. The application of high K+ solution is followed immediately by three consecutive washes using warm, aerated HEPES-PSS solution. Please click here to view a larger version of this figure.
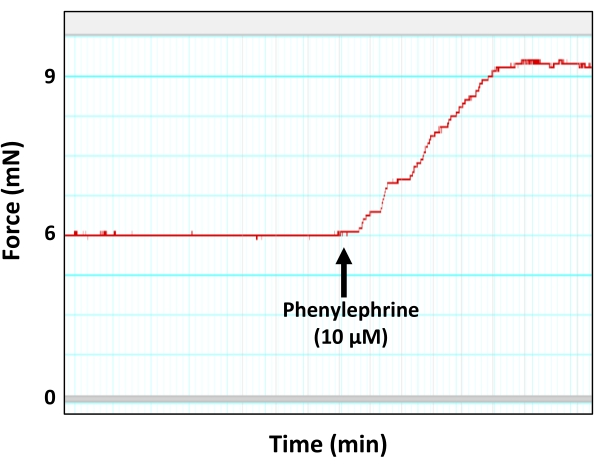
Figure 5: Aortic contraction in response to the vasoconstricting agent phenylephrine. Representative myograph trace showing force generation (contraction) by the aortic ring in response to the sub-maximum concentration of phenylephrine (10 µM). As shown, the peak of phenylephrine-induced contraction eventually reaches a plateau. Please click here to view a larger version of this figure.
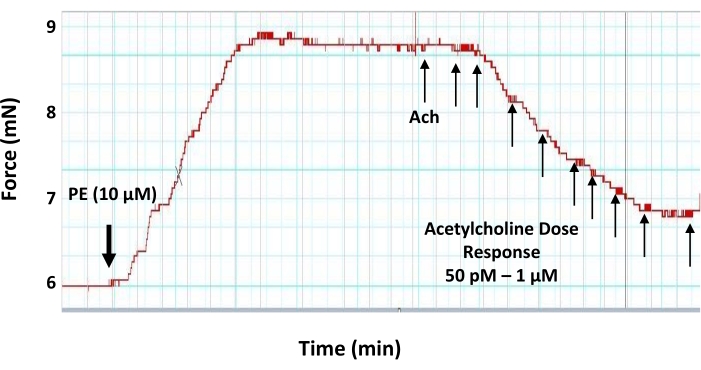
Figure 6: Dose-response effects of acetylcholine on the pre-contracted aortic ring. Representative myograph trace showing the dose-response (50 pM-1 μM) vasodilatory effect of the vasodilator neurotransmitter acetylcholine on a 2 mm pre-contracted aortic ring. The aortic ring is pre-contracted with 10 µM of phenylephrine prior to the application of acetylcholine. The first dose of acetylcholine is added when the phenylephrine-induced tension reaches a plateau. Please click here to view a larger version of this figure.
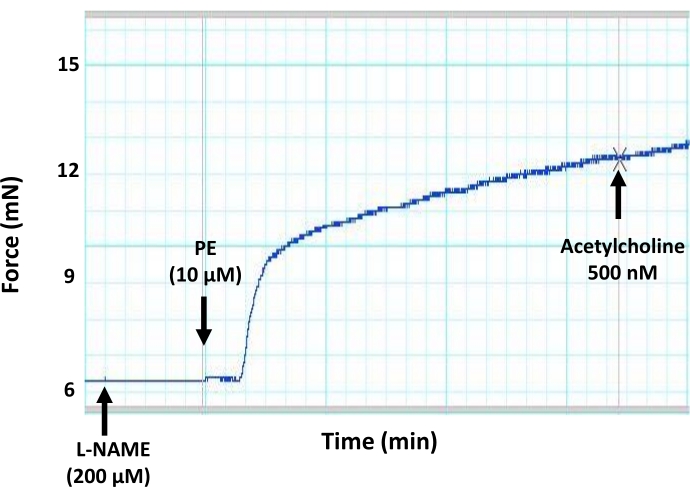
Figure 7: Effects of a general inhibitor of NO production (L-NAME) on endothelium-mediated vasorelaxation in mouse aorta. Representative myograph trace showing that the preincubation of aortic segments with a general inhibitor of NO production (L-NAME, 200 µM final concentration) blocks acetylcholine-induced vasodilation in a pre-contracted aortic ring. This is due to the inhibition of NO production by the endothelium due to the inhibitory action of L-NAME on eNOS. Acetylcholine was added to the pre-contracted aortic segment at the sub-maximum concentration of 500 nM. Please click here to view a larger version of this figure.
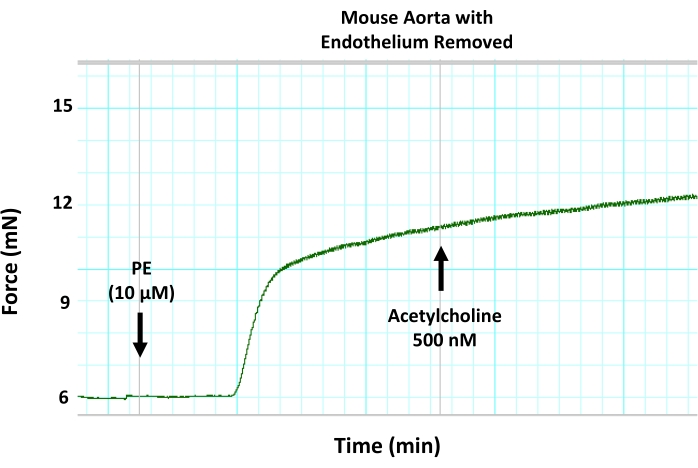
Figure 8: Effects of mechanical endothelium removal on endothelium-mediated vasorelaxation in mouse aorta. Representative myograph trace showing that removing the endothelium from aortic segments using wire denudation blocks acetylcholine-induced vasodilation in a pre-contracted aortic ring. This is due to the inhibition of endothelium-mediated vasorelaxation. Acetylcholine was added to the pre-contracted aortic segment at the sub-maximum concentration of 500 nM. Please click here to view a larger version of this figure.
