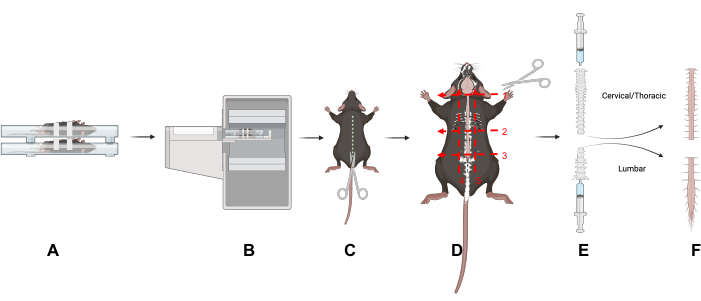
Figure 1: Study design. An overview of key techniques in this article. (A) Placing the mice in the scanning bed on their backs reduces motion in the spine. (B) PET/CT imaging of the mice. (C) Make an incision down the dorsal side of the animal to expose the spinal column. (D) Bisect the spinal column into cervical/thoracic and lumbar portions and remove the sections following the five indicated cuts. (E) Use a syringe to remove the spinal cord from the spinal column by making a seal with the syringe and spinal column and flushing from the cranial and caudal ends of the spinal column as shown. (F) Isolated cervical/thoracic and lumbar spinal cord segments. Abbreviation: PET/CT = Positron emission tomography/computed tomography. Please click here to view a larger version of this figure.
All animal studies were carried out in accordance with the Administrative Panel on Laboratory Animal Care (APLAC) at Stanford University, a program accredited by the Association for the Assessment and Accreditation of Laboratory Animal Care (AAALAC International). Mice were acclimated to the vivarium for at least 7 days prior to start of study to minimize stress on the mice, as stress can affect EAE induction.
1. EAE induction in female humanized CD19 mice
- Induce humanized CD19 C57BL/6J female mice aged 9-13 weeks with EAE as previously described5 using MOG1-125.
2. Animal care and scoring in EAE mouse model
- Score disease progression and care for the mice as previously described5. In brief, score this model on a scale of 1-5 as follows: 1 is tail weakness/limpness, 2 is weakened hindlimbs, 3 is hindlimb paralysis, 4 is hindlimb paralysis with forelimb weakness, 5 is moribund.
3. mAb conjugation, radiolabeling, and characterization
- Conjugate the bifunctional chelator 1,4,7,10-tetraazacyclododecane-1,4,7,10-tetraacetic acid mono-N-hydroxysuccinimide ester (DOTA-NHS-ester) to hCD19-mAb to radiolabel with 64Cu.
- Using a desalting column, exchange the hCD19-mAb storage buffer with HEPES buffer (pH 8.5-9): condition the desalting column(s) with HEPES. Calculate the number of columns needed based on desalting column sample volume capacity and volume of mAb required: 0.5 mL tubes: 30-130 µL of sample volume, 300 µL of wash; 2 mL tubes: 200-700 µL sample volume, 1 mL wash.
- Cool the centrifuge to 4 °C for buffer exchange via the desalting column.
- Retrieve the desalting column from the fridge. Remove the bottom of the desalting column, loosen the cap, and place the column in a collection tube.
- Centrifuge at 1,500 × g for 2 min to remove the storage solution; discard the flowthrough containing the storage solution and reuse the collection tube. Mark a line on the column where the highest point of the desalting compacted resin is slanted upward.
- Add HEPES buffer to the lower side of the desalting column. Place the desalting column in the centrifuge with the line facing outward; spin at 1,500 × g for 2 min. Discard the flowthrough and reuse the collection tube.
- Repeat steps 3.1.4 and 3.1.5 2x using the same collection tube and discarding the flowthrough between steps.
- Place the conditioned desalting column into a new collection tube and label; this tube will contain the hCD19-mAb.
- Add hCD19-mAb to the top of the conditioned desalting column(s) and use HEPES buffer to rinse the empty mAb vial; add this to the top of the desalting column (total volume as per the manufacturer's recommendation). Spin at 1,500 × g for 2 min to elute the hCD19-mAb. Keep the flowthrough containing the hCD19-mAb.
- Measure the concentration of hCD19-mAb using a UV/Vis spectrophotometer and adjust to 0.5 µg/µL with HEPES buffer if necessary.
- To the hCD19-mAb solution, add 1/50th the volume of the mAb solution of 0.5 M EDTA to make the final concentration of EDTA 0.01 M in the hCD19-mAb solution. Let the hCD19-mAb-EDTA solution stand at room temperature for 15 min.
- Remove the DOTA-NHS-ester from the freezer and allow it to come to room temperature (10-15 min). Calculate the volume of DMSO to add to the DOTA-NHS-ester to make a DOTA concentration that will allow the addition of the desired DOTA/mAb molar ratio (which is typically on the order of 1-2 DOTA/mAb).
NOTE: The volume of DMSO-DOTA-NHS-ester added to hCD19-mAb should not exceed 10% of the mAb volume. This should be done using a spreadsheet so it can be done quickly and repeatedly. - Based on the desired ratio of DOTA to hCD19-mAb, calculate the amount of DOTA-NHS-ester to add to hCD19-mAb.
nmol mAb × 10 DOTA/mAb → nmol DOTA → mg of DOTA → mg/mL DOTA/DMSO → mL of DMSO → dilution factor of DOTA/DMSO solution - Weigh 1-2 mg of the DOTA-NHS-ester, and carefully add the correct volume (calculated in step 3.1.11) of DMSO to the DOTA-NHS-ester; mix and spin down.
- Pipette the calculated volume of the DOTA-NHS-ester solution (step 3.1.12) into the hCD19-mAb solution; wipe the outside of pipette tip prior to addition to ensure extra DOTA-NHS-ester is not added (without changing the amount in the pipette). Gently mix and spin down.
- Place in the fridge (4 °C) to react overnight (12-16 h).
- Purification and concentration
- Cool the centrifuge to 4 °C for the centrifugal concentrator buffer exchange steps; place a metal PCR tube block on dry ice for snap-freezing the conjugate.
- Remove the DOTA-hCD19-mAb reaction from the fridge and quench by adding biological grade TRIS buffer: 10% of total reaction volume. Remove 10-20 µg of the sample for mass spectrometry analysis.
- Condition the desalting column(s) as described above (steps 3.1.1-3.1.5), using 0.1 M ammonium acetate buffer, pH 5.5.
- Buffer exchange the DOTA-hCD19-mAb solution to ammonium acetate (steps 3.1.1-3.1.8).
- Concentrate the DOTA-hCD19-mAb solution: add the solution to a 50 kDa molecular weight cut-off centrifugal concentrator following the manufacturer's recommendations on volume. Centrifuge at 4,000 × g for 10 min (or until the volume is reduced by 80%-90%); discard the flowthrough.
- Repeat nine more times (10 total): add enough ammonium acetate to bring the volume back to the maximum recommended volume.
NOTE: The total should be what was initially added, including what is left in the column, usually 400-450 µL for a 500 µL capacity centrifugal concentrator.- Rinse the reaction vial with ammonium acetate buffer to retrieve any residual DOTA-hCD19-mAb; add the wash to the centrifugal concentrator.
- Centrifuge at 4,000 × g for 10 min.
NOTE: The spin time may be reduced on subsequent spins if the volume is reduced to 80%-90% in less time.
- Remove the protein solution from the centrifugal concentrator. Note the total volume of the DOTA-hCD19-mAb.
- In centrifugal concentrator 2, add enough ammonium acetate buffer for a total volume of 100 µL and pipette to mix. Cap the centrifugal concentrator column and invert. Spin at 4,000 × g for 2 min to collect the solution. Transfer to a new tube.
- In centrifugal concentrator 500, use a pipette to collect the mAb solution from the centrifugal concentrator; add to a new tube.
- Measure the concentration using a UV-Vis Spectrophotometer. If the concentration is more than 2 mg/mL, dilute with ammonium acetate to 2 mg/mL.
- Aliquot 100 µg per PCR tube (approximately 50 µL); label the tubes with DOTA-hCD19-mAb, date, mass, and concentration. Spin down the vials.
- Snap-freeze the DOTA-hCD19-mAb on the chilled PCR block on dry ice (or freeze on dry ice). Once all the samples are frozen, place them in a -80 °C freezer.
- Measure the number of DOTA per hCD19-mAb by mass spectrometry. Keep a sample of unconjugated (pure) antibody from each conjugation to calculate the ratio. Use equation (1) given below; molecular weight is abbreviated MW.
 (1)
(1)
- Radiolabeling
NOTE: Wear appropriate personal protective equipment (PPE) for handling radioactivity, including a lab coat, gloves, and a personal body and ring dosimeters, following institutional regulations. Survey and change gloves regularly to prevent radioactive contamination. Use lead shielding and increase the distance from the radioactive source by handling with tongs when possible.- Transfer radioactivity from the shipping vial to a new vial using a pipette. Measure the radioactivity.
- Remove an aliquot for the first radiolabeling reaction. Add 50 µL of ammonium acetate (pH 5.5) per 1 mCi of 64Cu-CuCl3. Measure the pH by pipetting 1 µL onto a pH strip with a range that captures 5.5 with enough resolution to distinguish between 5 and 6.
- If the pH is not 4-5.5, alter it using 1 M NaOH or 0.1 M HCl. Add small amounts, 1-5 µL, of 1 M NaOH if pH is less than 4 or 0.1 M HCl if pH is greater than 5.5 until the correct pH is reached. With each addition, mix thoroughly, spin down, and measure the pH as described above. Note each addition and removal of any solution (including to check the pH) so the final volume can be calculated.
- Once the optimal pH has been achieved, add 10 µg of DOTA-hCD19-mAb per 1 mCi of 64Cu-CuCl3. Mix gently and spin down briefly.
- Place the reaction vial on a thermomixer set to 37 °C and 400 revolutions per minute (rpm).
- After 30 min, quench the reaction: divide the total reaction volume by 50, and add that volume of 0.5 M EDTA to the reaction mixture.
- Determine the labeling efficiency using instant thin layer chromatography (ITLC) to measure the percentage of bound and free copper in the solution.
- Cut 1 cm-wide strips of TLC paper. Mark 1 cm from the top and bottom of the strip and prepare a tube (50 mL conical flask) with mobile phase less than 1 cm of 0.1 M citric acid (the level of mobile phase should be below the 1 cm mark on the strip when placed in the tube).
- Pipette 1 µL of the reaction solution on the strip at the bottom 1 cm mark (solvent front) and place the strip in the tube. Watch until the solvent front reaches the top 1 cm mark, remove the strip, and wrap it in a piece of plastic wrap.
- Place the strip on the platform and run it through a radio-TLC imaging scanner. Look for the radiolabeled mAb at the origin and free 64Cu that travels with the mobile phase front (Figure 2). If the percentage of free copper is less than 5% (95% labeling efficiency), proceed with injection into animals. If the percentage of free copper is greater than 5%, proceed with purification.
NOTE: The percentage of free copper generally depends on the ratio of DOTA-mAb to 64Cu, reaction time, pH, and temperature. The reaction conditions should be optimized by each user for each new mAb to ensure consistent results.
- Purification via a disposable DNA grade gravity column
- Condition a disposable DNA grade gravity flow column (desalting/buffer exchange column) according to the manufacturer's directions. Place the disposable DNA grade gravity column on a ring stand or other instrument behind adequate lead shielding; ensure the apparatus is stable and easily movable. Place the tube underneath the column.
- Pipette the crude reaction mixture onto the gravity flow column resin. Wait until all the liquid has flowed into the resin. Pipette sufficient PBS to bring the entire volume (crude product plus PBS) to 500 µL. Dispose of the flowthrough.
- Place the column over 1.5 mL centrifuge tubes labeled 1-10. Add 1 mL of PBS to the column. Collect five drops in each tube until the flow has stopped.
NOTE: Fewer than 10 tubes may be required. - Cap the bottom of the column and measure the residual radioactivity. Measure each vial with flowthrough. For each vial with more than 50 µCi, prepare an ITLC per step 3.3.7 to measure the percent bound copper in each fraction.
NOTE: The first one or two fractions will contain only mobile phase; the radiolabeled mAb will elute first (typically fractions 2 or 3 through 5 or 6) and the free 64Cu will elute last (some will stick to the column). The percent bound 64Cu may vary between fractions. - Combine the fractions with greater than 95% binding (less than 5% free copper); use the solution for injection. If desired, perform size-exclusion HPLC to confirm radiolabeling5 and calculate the molar activity. Save an aliquot to measure the concentration on a UV-Vis spectrophotometer after it has decayed 10 half-lives (127 h or 5.3 days).
4. Dose preparation
NOTE: Before handling the dose, wear proper PPE, including lab coat, body and finger dosimeters, and gloves.
- Inject 64Cu-DOTA-hCD19-mAb 18-24 h prior to PET scanning, to allow adequate circulation of the radiotracer in the body.
- Immediately place the lead container with the 64Cu-DOTA-hCD19-mAb behind lead shielding. Turn on the Geiger counter to monitor potential contamination.
NOTE: Change gloves frequently when handling radioactive material. Double-gloving while drawing doses is recommended to facilitate swift glove changes. Always place contaminated sharps and trash in the designated shielded trash area. - Dilute the 64Cu-DOTA-hCD19-mAb to an appropriate concentration in a low bind 1.5 mL plastic centrifuge tube.
NOTE: The 64Cu-DOTA-hCD19-mAb will bind to plastic if it is not low bind; 64Cu will bind to glass.- Dilute the radiotracer in saline to prevent radiolysis and simplify drawing consistent doses.
- Prepare doses to administer between 75 and 150 µCi in 100 µL, if possible. Ensure that the maximum total injected volume does not exceed 10% of the mouse's body weight.
- Use a 500 µL (50 cc) insulin syringe to draw the dose from the low bind plastic tube. Ensure there are no bubbles in the syringe since it will be injected intravenously.
- Prelabel the syringes with the corresponding animal numbers.
- Record the dose activity and time in a lab notebook for data analysis.
- Have the doses ready for injection as soon as the animals are catheterized to reduce time under anesthesia.
- After the doses have been prepared, prepare a standard (phantom) for scanning to generate a calibration factor.
- Fill a 15 mL conical tube with 50-75 µCi of activity diluted in water (or PBS).
NOTE: Ensure thorough mixing of the solution. The standard can be free 64Cu left over from labeling.- Measure the amount of activity in the standard and record the time.
- Fill a 15 mL conical tube with 50-75 µCi of activity diluted in water (or PBS).
5. Cannulation and Injection
NOTE: See previously described methods6 for intravenous cannulation of mice for injection of the radiotracer6.
- Weigh and score the mice for disease severity as described in section 2.1 before anesthetizing mice in a knockdown box filled with 1.5-3% isoflurane in preparation for radiotracer administration.
NOTE: These mice will be injected on the bench top, not on the PET scanner as previously described. There is no need to glue the catheters in place for injection, as the mice will not be moved between cannulation and injection. - Once a mouse is cannulated, insert the needle into the end of the catheter and inject slowly. After injection, follow with a small saline flush through the catheter to ensure the entire dose is injected.
NOTE: The volume should approximately equal the dead volume of the catheter, which is 50 µL for the catheters used by the authors.- Inject over a piece of laboratory wipe to collect any drips of radiotracer; include this when measuring the residual dose.
- Record the time of injection in a lab notebook.
- Remove the cannula immediately after injection. Measure the cannula, dose syringe, and tissue using a dose calibrator to determine the residual dose that was not injected into the mouse.
- Record the activity and time in a lab notebook.
- After the mice are injected, label their cages with a cage card indicating the mice are radioactive. Record and log the cages according to institutional guidelines. Then, place the mice in a designated radioactive holding area.
6. PET/CT imaging
- Perform PET imaging 18-24 h after the injection of 64Cu-DOTA-hCD19-mAb. Weigh and score the mice prior to scanning.
NOTE: The scanner operating instructions depend on the scanner being used.- Ensure the X-ray component of the PET/CT scanner is warmed up and ready for acquisition.
- Open the PET scanner acquisition software on the computer.
- From the Investigator Login dropdown menu, click on the appropriate lab information.
- On the Project page, either create a new project or select an existing project from the dropdown menu.
- When the Initialization prompt automatically appears on the screen, click on Home Bed and wait for bed to home. Then, click on Warm up CT.
- Ensure the CT shielding door is closed to allow the CT to warm up.
- While the scanner is warming up, score the EAE mice and inject them subcutaneously with 0.2-0.4 mL warm saline in the flank for hydration.
- After the scanner is warmed up, go back to the computer to set up the PET scans for the study.
NOTE: These can be set up prior to the day of scan.- Under the Recent Studies header, click on Create New Study. Fill out the study name, protocol, compound, and subject information.
- If performing a PET/CT, select PET Protocol first, and then select CT Protocol.
NOTE: Typically, a standard CT is sufficient for scanning the EAE mouse model. A CT scan is 1 min long and acquired with binning at 2 x 2 at voltage 80 kVp, current 150 µA, and 720 projections. CT images are reconstructed using a Modified Feldkamp Algorithm. - For the PET protocol, choose a 10-15 min static 64-copper scan. If this scan is not already on the list of available protocols, add it by clicking on the Protocols tab in the Standard menu, Create New Protocol | Isotopes dropdown menu. If the desired isotope is not listed, click on More | Add from Library and add the desired isotope. Define the scan duration, click on the radio button for Static Scan, name the protocol and click on Save.
- Return to the Studies tab and continue to name and set up all the desired scans for the day.
NOTE: It is recommended to also set up one "CT Test" scan using only a standard CT to check the bed positioning of the first scan to ensure optimal placement. This should be the first scan run for the study.
- If performing a PET/CT, select PET Protocol first, and then select CT Protocol.
- Under the Recent Studies header, click on Create New Study. Fill out the study name, protocol, compound, and subject information.
- Once the scanner is ready, anesthetize the mice in a knockdown box to prepare them for the scan.
NOTE: At this stage, the mice are likely very sick; it is best practice to minimize the time under anesthesia.- Apply eye gel.
- Ensure the four-mouse scanning bed is equipped with heating elements, such as heating pads or heated air, with isoflurane set to 1.5%-2% and heating pad turned on (Figure 3). Place the mice in a supine position on the scanning bed.
- As EAE disease progresses, the spine of the mouse becomes severely curved. Scan the mice while they are on their backs to straighten the spine as much as possible, improving the analysis downstream. Gently pull the mouse tail to aid in straightening the spine.
- Once in the supine position, securely tape each mouse in place with soft microscope tape. Use one strip of tape over the head and another gently over the belly to minimize motion due to breathing.
- Record in a lab notebook which mouse is in what scanning position.
- Once the mice are secured, return to the scanning computer to operate the scanner.
- Open the Motion Controller menu. Click on PET Center FOV to move the mice on the scanning bed into the PET ring. For the first scan of the day, click on CT Center FOV. Once in position, run the CT Test scan to ensure the position is correct; repeat until the bed position is satisfactory.
- Place a small piece of white tape on the scanning bed to mark the correct bed placement for the remainder of the study.
- Once the bed is in place for the PET scan, initiate the scanning sequence by clicking on Run.
- Wait for the scanner to automatically move from the PET ring to the CT.
- Always visually check whether the animals have moved into the proper position for both PET and CT.
- Record the scan start time in a lab notebook for decay correction of the dose injected during data analysis.
- After the scan is complete, allow the image to reconstruct. Check the data before removing the animals.
NOTE: 3D-ordered subsets expectation-maximization (OSEM) reconstruction will take approximately 5 min for a static scan. - Visually check and approve the data, using the spleen as a positive control as this tissue contains a large number of B cells. Remove the animals from the scanning bed and place them in an isoflurane-filled knockdown box in preparation for perfusion and subsequent dissection.
- Repeat steps 6.5-6.12 for the remaining mice in the study.
- When all the mice are scanned or when scanning a group that has an open place in the scanning bed, scan the standard prepared in step 4.6.
7. Dissection for ex vivo gamma counting and autoradiography
- Before dissecting, ensure all gamma counting and centrifuge tubes have been pre-weighed.
- Perform euthanasia via perfusion, as previously described6, with PBS and thoracotomy while the mice are deeply anesthetized (continual inhalation of 4% isoflurane, 2 L/min 100% O2).
- To remove the bone marrow, cut both femurs at the knee and pelvis. Make sure both heads are removed from the femur.
- Place both femurs in a 0.5 mL centrifuge tube that has a hole at the bottom (using a 20 G needle) and has the lid cut off.
- Place the 0.5 mL tube containing the femurs inside a 1.5 mL centrifuge tube with the lid cut off.
- Place the entire tube setup in a mini centrifuge. Spin for 4 min at 4,500 × g.
NOTE: The bone marrow should be dislodged through the hole in the 0.5 mL centrifuge tube and settle at the bottom of the 1.5 mL centrifuge tube.- Separate the tubes. Weigh the empty femurs in the 0.5 mL centrifuge tube. Weigh the bone marrow in the 1.5 mL centrifuge tube. Place each centrifuge tube in gamma counting tubes.
- Remove the brain using forceps and scissors, taking care to keep the brainstem intact. Place the brain in a gamma counting tube. Record the dry weight, flush with PBS, and keep on ice until ready for counting.
- To remove the spinal cord, perform the following steps.
- Remove the skin and fur by making an incision down the dorsal side of the animal to expose the spinal column (Figure 1).
- Separate the lumbar (L) from the cervical (C) and thoracic regions by cutting along three transverse planes around and through the spinal column: at the base of the neck (C1 vertebra) (Figure 1D, Number 1); at the base of the ribcage (L1 vertebra) (Figure 1D, Number 2); at the base of the pelvis (L5 vertebra) (Figure 1D, Number 3).
- Cut under the rib cage (Figure 1D, Number 2).
- Cut directly above the sacrum to separate the lumbar spinal region. Carefully trim the spinal column from the pelvic end until the lumbar spinal cord is visible (Figure 1D, Number 3). Trim off the surrounding tissues to isolate the lumbar and cervical/thoracic regions of the spinal column (Figure 1D, Numbers 4 and 5).
- To expel the spinal cord, use a slip-tip syringe (3-10 mL) filled with PBS. Create a seal between the syringe and the spinal column using the thumb and forefinger.
- Gently push the PBS through the syringe to expel the spinal cord onto an absorbent pad (Figure 1E); repeat for both spinal regions. Place the spinal cord tissues in a gamma counting tube.
- Record the dry weight, and add PBS to ensure the tissue is at the bottom of tube to avoid drying. Place the tube on ice until ready for counting.
- Expel the cervical/thoracic spinal cord from the cranial end and the lumbar spinal cord from the caudal end of the spinal column (Figure 1E).
8. Ex vivo gamma counting
- Open the gamma counter software. Navigate to the work list and select the desired protocol, such as a 30 s counting protocol for 64Cu.
- Prepare at least three standards in separate tubes. Run them now for use in analysis (step 10.2). Aim to make three replicate volumes and amounts of activity in three separate tubes.
NOTE: A volume of 500 µL gives good results. While activity will be determined by the machine used, 10 µCi generally works well. - Place the standards in a rack labeled with the barcode corresponding to the desired protocol to be run. Place the rack on gamma counter.
- After recording the organ weights, place the tubes containing the organs on the gamma counting rack after the tubes containing the standards.
NOTE: Organs of interest for this model can include axial lymph nodes, blood, bone marrow, brain, cervical lymph nodes, femur, heart, liver, lumbar spinal cord, muscle, spleen, tail, and cervical/thoracic spinal cord. - Put a rack with a stop barcode in the back of the gamma counter.
- Press the Play button on the computer. If possible, do not press Play until there are multiple racks or organs to be run to allow all tubes to be continuously counted in one file. Ensure that a rack with a stop barcode is in the back of the gamma counter for each run.
- Run until all the samples have been counted. Save and export the file.
9. Ex vivo autoradiography (ARG) of CNS tissue
- Follow previously published steps for both brain and spinal cord ARG (while excluding steps 2-6 described by Chaney et al., as the mice are already injected with radiotracer from the PET scan)6.
NOTE: Specific instructions for preparing the spinal cord ARG cassette are listed here6. - After gamma counting is complete for the lumbar and cervical/thoracic spinal cords, promptly place the tubes on ice until all CNS tissues have been counted.
NOTE: Refer to the previously published method for ARG of the brain6. - Gently tip the tubes to allow the spinal cords to fall out onto an absorbent pad. If the spinal cord sticks to the side of the tube, gently flush with cold PBS and tip the tube again. Carefully dry each spinal cord by gently blotting with a lab tissue. Place the dried spinal cords in an organized fashion on a thick black piece of paper.
- Label next to the spinal cords with a white pen for easy identification.
- Leave space at the corners and in the middle of the black paper to place stacks of three microscope slides to act as spacers to prevent the compression of the spinal cords when the ARG cassette is closed. Use 5-7 stacks.
- Once all the lumbar and cervical/thoracic spinal cords are positioned on the black paper and labeled, carefully place the piece of paper in the ARG cassette. Place the open cassette on a tray of dry ice to freeze the spinal cords.
- Once frozen, gently place plastic wrap between the digital phosphor storage screen and the spinal cords and place the screen on top of the samples. Immediately close the cassette and place it in the -20 °C freezer for approximately 10 half-lives (~127 h).
- When the exposure time is complete, scan the film using a phosphor imager. Analyze the resulting digital image (see section 12 for instructions).
10. Analysis of biodistribution data
- Set up a "Dose Correction" spreadsheet to mathematically determine the time correction for the radioactive decay, thus normalizing radiation doses and allowing comparisons between subjects.
- Decay-correct all doses to the injection time, accounting for residual activity left in the syringe and catheter after injection.
- Using the standards prepared in step 8.2, average the activity amount (µCi) and normalized counts per minute (CPM). Divide the average CPM by the average standard activity amount to get CPM/µCi.
NOTE: Ensure the activity amount for each standard is decay-corrected to the time the gamma counter counts the CPM of the standards. The gamma counter should normalize all CPM values to the start time of the protocol.
- Set up the "Results" spreadsheet to calculate the final percent injected dose per gram of tissue (%ID/g) for each sample.
- Decay-correct the normalized CPM from the gamma counter for each sample counted to the injection time of the animal.
NOTE: Decay correction can be to any time point; ensure all doses and CPM values are decay-corrected to the same time point. - Normalize the decay-corrected CPM to the mass of each sample to determine the CPM per sample. Calculate the total CPM injected by subtracting the CPM in the tail from the calculated injected CPM.
NOTE: The tail does not need to be mass-corrected as this CPM value will simply be subtracted from the total injected CPM to account for any extravenous tracer from injection. - Divide the CPM per mass by the total CPM injected to calculate %ID/g.
- Decay-correct the normalized CPM from the gamma counter for each sample counted to the injection time of the animal.
- Set up a "Summary" spreadsheet to display the final results for input into a graphing software and subsequent data visualization and statistical analysis.
11. PET image analysis
- Open the PET analysis software. lick on File |Open Local Data | DICOM. Locate the desired file (DICOM format). Open both the PET and CT.
- In the Data Manager, adjust the PET and CT contrast to the desired levels.
- Register and crop individual mice.
- In the Navigation menu, select the Reorientation/Registration tab.
- Go to the Rigid menu within this tab. Designate the CT scan (0) as the Fixed scan and the PET scan (1) as the Moving scan.
- Select Rigid Transformation and Fast Quality. Click on Anmelden.
- After registration is complete (5-10 min), click on the check mark to save the registration.
- Visually inspect the data to ensure registration was successful. Export the session by clicking on File | Session | Export.
- Next, crop each mouse in a full body crop: go to the Navigation menu and click on Cropping. Drag the sides of each cross section from the outer edge inward.
- Once the desired mouse is tightly cropped, click on the check mark, and export the session to save.
- Next, crop and straighten the heads of each mouse for brain analysis using the manual Translation, Rotations, and Flips in the Registration/Reorientation menu. Export to save.
- Analyze the spinal cord.
- To begin analysis of regions of interest (ROIs) in the spinal cord, open the 3D ROI Tool from the Navigation Menu.
- Under the ROIs header, use the plus sign at the bottom of the menu to create six ROIs: Lumbar ROI, Cervical/Thoracic ROI, Lumbar Skeleton, Thoracic Skeleton, Lumbar Spinal Cord, Thoracic Spinal Cord.
NOTE: The Lumbar and Cervical/Thoracic ROIs are generalized large ROIs that will be used to create the skeleton ROIs (Figure 4). - To avoid visual interference from the PET signal with this step, click on F3 to turn off the PET.
- Go to the top of the 3D ROI Tool Operator. Click on the solid dot to the right of the cursor symbol to open the 3D Paint Mode and Erode/Dilate menu.
- Select Sphere and change the size auf 20 pixels. Set Dilate auf +5.
- Before proceeding, go to the bottom of the menu. Ensure the Lumbar ROI is selected, as this is the first ROI to be drawn.
- On the CT, find the L6 vertebra of the spinal column (where the spine meets the hips). Starting one vertebra above L6, draw a rough ROI Lumbar ROI over the five vertebrae above the hips (L1-L5 vertebrae). Then, switch to Cervical/Thoracic ROI and trace the remainder of the spine to the base of the skull.
NOTE: This does not have to be precise, as it is used to indicate where Otsu thresholding should occur in step 11.4.8. - After drawing the generalized ROIs, go to the top of the operator. Select the Segmentation Algorithms menu.
- From the dropdown menu, select Otsu Thresholding. For the input, select Lumbar ROI. At the bottom of the menu, ensure Lumbar Skeleton is selected. In the dropdown menu next to Image, ensure the CT scan is selected and click on Apply. Repeat for Cervical/Thoracic ROI and Thoracic Skeleton.
- If the Otsu Thresholding does not sufficiently highlight the spinal column, use Global Thresholding and change the Min value to 350 and the Max auf 3,500 for manual thresholding and adjust as necessary to isolate the vertebrae.
- After using Otsu Thresholding to create the Skeleton ROIs, return to the Navigation menu (cursor icon). Either delete or checkmark the H (hide) column for both the rough Lumbar and Cervical/Thoracic ROIs to hide them. Checkmark the I (immutable) column for both Skeleton ROIs so they cannot be edited.
- Finally, return to the top of the 3D ROI Tool Operator and go to the 3D Paint menu to draw the Spinal Cord ROIs.
- Select the Sphere tool again and trace the spinal cord within the skeleton for both Lumbar and Thoracic, ensuring the correct ROI is selected at the bottom of the menu.
- To erase any ROI, click on Command/Control and draw over the part to be erased.
- Check the spinal cord ROI from all three planes to make sure there is no ROI drawn outside of the spinal column.
- Export spinal cord analysis results.
- If the PET signal was turned off in step 11.4.3, press F3 after the Spinal Cord ROIs are drawn to turn the PET back on, or select the Visual Controller (VC) and click on the PET bar.
- Go back to the Navigation menu (cursor icon). Click on the grid icon to Show Table. Copy the table into spreadsheet software and save.
- Lastly, export the file in PET analysis software, as described above, to save the ROIs drawn.
- Analyze the brain using a semi-automated 3D atlas.
- Open the head crop file. Import the mouse brain atlas by going to the Advanced Modules menu and selecting the 3D Brain Atlas Tool. Make sure the reference is set to CT and the crop option is unchecked. Set a pathway for the output directory.
- In Advanced Setting, change Transform auf Versor-Affine. Keep all other default settings. Click on Run.
- Manually adjust the atlas in the Reorientation/Registration menu and use the CT of the skull as a guideline for fitting the atlas.
- Use great care if scaling is necessary, as this can greatly affect brain structure volumes. Click on the checkmark when adjustment is complete.
- Rerun the atlas with Import 3D ROIs selected.
- Export the file to save the atlas fitted to the cropped head.
- After drawing and exporting all ROIs from the desired organs, calculate a standard binding correction value. Decay-correct all data and convert to %ID/g as previously described6. Normalize to the organ that suits the animal model, such as the heart to normalize to radiotracer present in the blood pool.
12. Ex vivo autoradiography analysis
- Open the digital image file (.gel) using the image analysis software. Adjust brightness and contrast to the desired threshold. Apply a suitable color lookup table if desired.
NOTE: Royal or Grays are recommended for ease of visualization.
The hCD19-mAb was DOTA-conjugated and radiolabeled with 64Cu as shown in Figure 2. EAE and naïve mice underwent PET/CT scanning (Figure 3) 18-24 h after injection with 64Cu-DOTA-hCD19-mAb. PET/CT images were co-registered using the PET analysis software, and the CNS tissues were analyzed using manual ROIs or a semi-automated 3D brain atlas. Radiotracer binding in ROIs (Figure 4) was higher in EAE mice than in naïve mice. Ex vivo gamma counting and ARG showed increased binding in the spinal cord (both lumbar and cervical thoracic segments) and brain (ARG only) of EAE mice compared to naïve (Figure 5 and Figure 6). Ex vivo gamma counting of perfused mice also showed decreased radiotracer binding in peripheral organs, including spleen, femur, and bone marrow (Figure 5), consistent with B cells leaving the periphery and infiltrating the CNS in this EAE model.
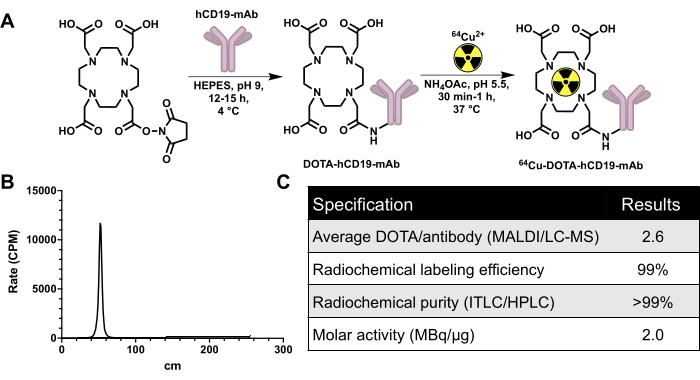
Figure 2: Conjugation and radiolabeling scheme for generating 64Cu-labeled human-specific CD19 monoclonal antibody, 16C4-TM mAb (64Cu-DOTA-hCD19-mAb), in addition to quality control data. (A) Reaction of DOTA-NHS-ester with hCD19 monoclonal antibody to produce hCD19-DOTA conjugate (not to scale) and radiolabeling with 64Cu-CuCl3 to produce 64Cu-DOTA-hCD19-mAb. (B) Representative ITLC chromatograph. The peak at 40-60 cm is the radiolabeled antibody; unbound 64Cu-CuCl3 travels with the mobile phase and would be present from 200 to 240 cm. There is no detectable free 64Cu-CuCl3 in this chromatograph. (C) The quality control specifications of the radiolabeled antibody. Abbreviations: DOTA-NHS ester = 1,4,7,10-Tetraazacyclododecane-1,4,7,10-tetraacetic acid mono-N-hydroxysuccinimide ester; ITLC/HPLC = instant thin layer chromatography/high-performance liquid chromatography; MALDI/LC-MS = matrix-assisted laser desorption/ionization/liquid chromatography-mass spectrometry; CPM = counts per minute. Please click here to view a larger version of this figure.
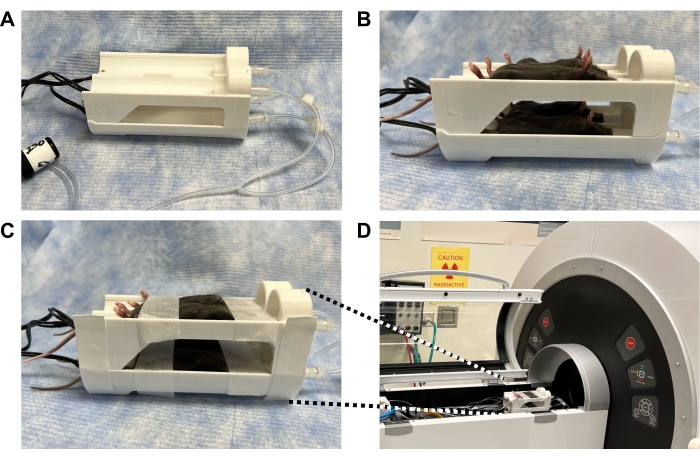
Figure 3: Photographs demonstrating how to secure mice in a 3D-printed bed within the PET scanner to enable high quality imaging of the spinal cord and brain while minimizing motion. (A) 3D printed four-mouse scanner bed (also known as "mouse hotel") equipped with heating elements and anesthesia tubing. (B) Anesthetized mice in a supine position to maximize straightness of the spine; the bed position of each mouse is recorded. (C) Mice taped securely across their head to minimize motion in the brain and across the belly to minimize motion from breathing, without affecting breathing. (D) Mouse bed positioned within the scanner and taped to the scanning bed. Anesthesia tubing was connected from scanner to bed and isoflurane set to 2%. Mouse breathing was monitored to ensure appropriate isoflurane level before closing the scanner door. Abbreviation: PET = Positron emission tomography. Please click here to view a larger version of this figure.
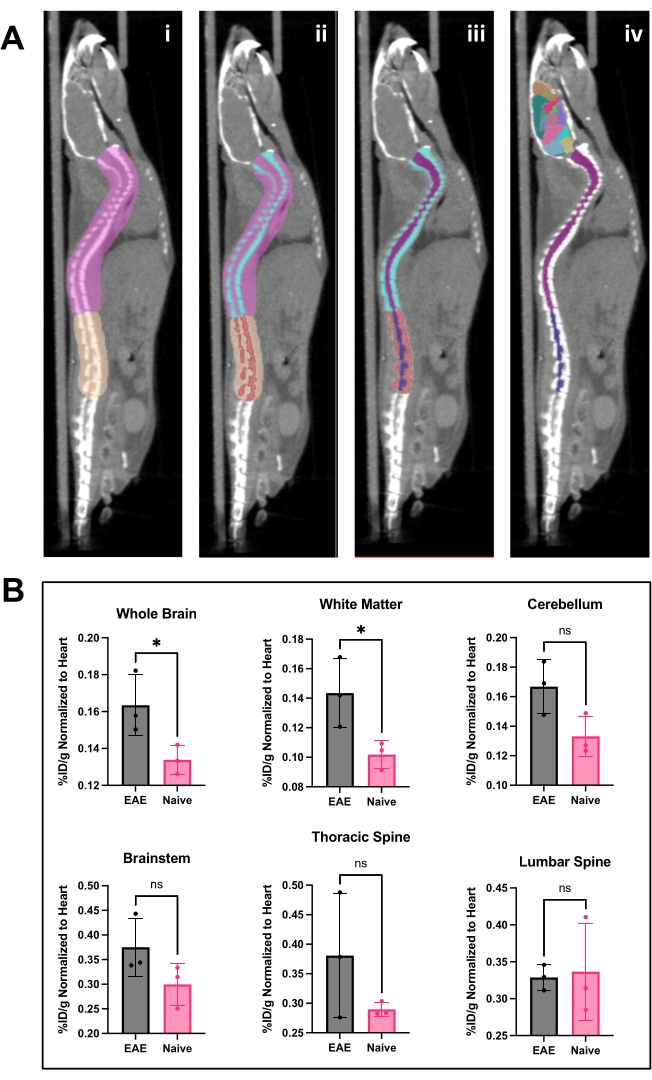
Figure 4: Spinal cord image and brain analysis and results using PET analysis software. (A) i) ROIs (pink and tan) drawn on spine to separate lumbar from the thoracic and cervical vertebrae and prepare image for Otsu thresholding. ii) Spinal vertebrae (turquoise and red) were segmented out using Otsu Thresholding. iii) Vertebrae were then made immutable in the 3D ROI menu, and the spinal cord divided into cervical/thoracic (purple) and lumbar (navy) ROIs. iv) The vertebral ROI was removed, leaving spinal cord ROIs and representative brain atlas applied. (B) Representative analysis of PET results from various CNS regions represented as %ID/g normalized to the ROI of the heart within each animal. PET acquisition was a 10 min static scan via PET/CT imaging. Brain regions quantified using a semi-automated brain atlas approach, shown in panel A. iv) Representative results show either significance or trending toward significant increase in tracer binding in the brain and thoracic spinal cord. Statistics performed using Student's t-test (*: p < 0.0332). Abbreviations: PET = Positron emission tomography; ROIs = regions of interest; CNS = central nervous system; CT = computed tomography; %ID/g = percent injected dose per gram of tissue; EAE = experimental autoimmune encephalomyelitis. Please click here to view a larger version of this figure.
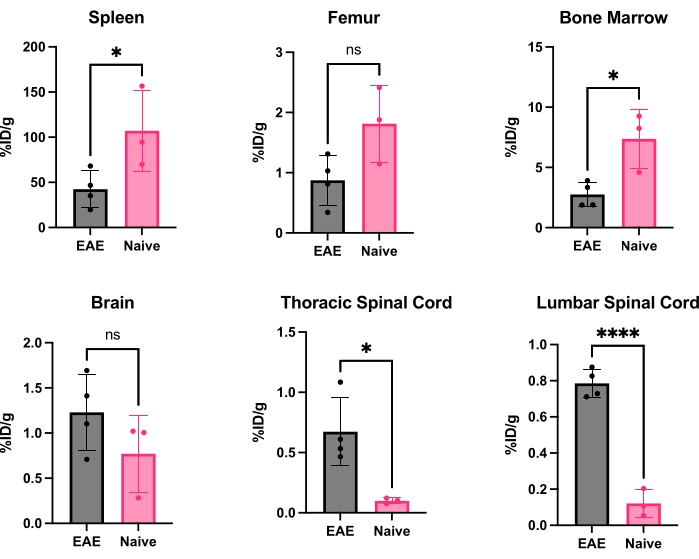
Figure 5: Representative quantification of ex vivo gamma counting in various organs in EAE and naïve mice expressed as %ID/g. Post-PET scan, mice were perfused with PBS to remove the radiotracer present in the blood, either free or bound to blood-resident CD19+ B cells, and organs quickly dissected and weighed to have an accurate weight of each organ. Tracer binding is significantly decreased in the spleen and bone marrow in EAE mice compared to naïve ones. Increased radiotracer binding is observed in both the lumbar and cervical/thoracic spinal cord segments of EAE mice. The brain does not show significant increase in radiotracer signal, though it is trending toward significant increase. Statistics performed using Student's t-test (*: p < 0.0332; ****: p < 0.0001). Abbreviations: PET = Positron emission tomography; %ID/g = percent injected dose per gram of tissue; EAE = experimental autoimmune encephalomyelitis; PBS = phosphate-buffered saline. Please click here to view a larger version of this figure.
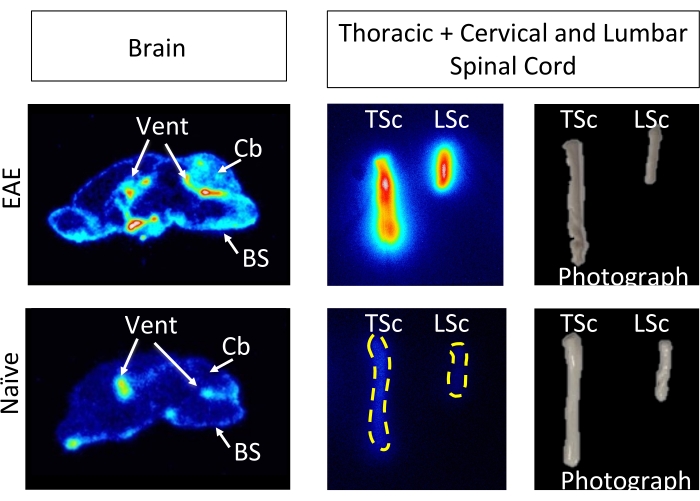
Figure 6: Ex vivo ARG images depict 64Cu-DOTA-hCD19-mAb binding in sagittal brain sections and whole spinal cords from EAE compared with naive mice. Digital phosphor storage films were scanned using a phosphor imager after being exposed to radioactive tissue samples for approximately 10 half-lives (127 h or 5 days). The resulting images reveal visually higher signal in the brain of EAE mice compared to brain sections from naïve mice, which is expected due to the regions known to contain B cells in this model5. Specifically, there is increased tracer signal in the brain stem, cerebellum, and ventricles of EAE mouse brain sections. This increase in signal for EAE mouse brain sections mirrors what was found for in the whole-brain PET quantification detailed above. Similarly, there is an increase in radiotracer binding in both the cervical/thoracic and lumbar spinal cord segments compared to naïve spinal cords, reflecting what was found using ex vivo gamma counting. Abbreviations: PET = Positron emission tomography; EAE = experimental autoimmune encephalomyelitis; Vent = ventricles; Cb = cerebellum; BS = brain stem; TSc = thoracic and cervical spinal cords combined; LSc = lumbar spinal cord. Please click here to view a larger version of this figure.
Supplemental Figure S1: Staining of CNS tissues of naïve and EAE mouse brain tissue with CD45R/B220. B cells are observed in brainstem, meninges, and white matter of EAE mice (n = 7 EAE, n = 5 naïve mice, average four slices per animal). This figure is from 5. Scale bars = 5 mm (low magnification [1x]) in sagittal brain images, 100 µm (high magnification [20x]) in brainstem, meninges, and cerebellar white matter. Please click here to download this File.
