The research was conducted in three different Italian Centers: Humanitas Research Hospital – Gavazzeni (BG), Montallegro Clinic (GE), and Biomedical Institute (GE) from February 2020 to February 2021, and approved by the hospital's Ethical Committee or Internal Review Board (IRB). The research was conducted in respect of the Helsinki rules for human rights and GCP. All patients were informed about the risk of the procedure and signed a written consent before being included in the study. Refer to Supplementary File 1 for the overview of the procedure.
1. Preparation
- Prepare the room and the operating table with all the materials listed in the Table of Materials. As it is commonly used in human surgical interventions, all the materials are packaged and sterilized at the origin by each manufacturer.
- Place 5% dextrose solution into a bowl and immerse a 3 mL and a 10 mL syringe, a needle (18 G), and either a 1 mL or 2 mL vial (see step 3.2.5) containing NBCA+MS surgical glue.
2. Anesthesiology technique and surgical preparation of the patient (Figure 1)
- Completely depilate the leg to be treated, from the groin to the foot.
- Disinfect the leg to be treated with an alcoholic solution of 2% chlorhexidine di-gluconate.
- Perform an ECD in the orthostatic and clinostatic positions. Set the instrument through the manufacturer's software, which provides various presets.
NOTE: The venous vascular preset is used for this procedure, and the ultrasound probe is set at 7.5 MHz.- First, position the patient upright on a step in front of the operator and map the entire venous vascular tree through the ultrasound probe.
- Subsequently, place the patient on the operating table in the supine position and perform the vascular scanning again. This preoperative procedure is necessary for a complete clinical evaluation of the vessels.
- Map out the pathway of venous incompetence on the skin through ECD using a dermographic pen (Figure 1).
- Place the patient in the supine position for GSV treatment or the prone position for SSV treatment.
- Disinfect the leg again with an alcoholic solution of 2% chlorhexidine di-gluconate.
- Prepare the sterile field with a surgical drape.

Figure 1: Preparation steps. On the right side, the figure shows the operating table preparation with the tools needed for the procedure, such as disinfectant, 5% dextrose solution, syringes, and an NBCA+MS surgical glue vial. The figure shows a schematic mapping of venous incompetence on the left side. Specifically, this is carried out under ECD guidance using a dermographic pen directly on the patient's skin. Please click here to view a larger version of this figure.
3. Surgical technique
- Time of vascular study (Figure 2)
- Perform the ultrasound-guided study of the lengths and diameters of the veins to be treated as described in step 2.3. Place the patient in the clinostatic position and perform the vascular study through the ultrasound probe.
- Evaluate the reflux time (RT) with the ultrasound, which defines the degree of incompetence of the terminal valve. The physiological values of RT are 0.1 s < RT < 0.5 s, while RT > 0.5 s indicates a pathological condition4. Carry out the classification of severity by evaluation of the Galeandro quartile11.
- Using the ECD, identify the junction between the epigastric vein and preterminal valve for the treatment of the GSV (Figure 2), or the saphenous-popliteal junction for the treatment of the SSV.
- Operative time (Figure 3)
- Induce local anesthesia with 1-1.5 mL of 10 mg/mL mepivacaine in the area of needle insertion.
- Perform ultrasound-guided catheterization of the saphenous vein (GSV/SSV) according to the Seldinger technique12 (using an angiographic needle, a guidewire, and an introducer) 14-16 cm downstream of the relevant junction (Figure 3A).
- Percutaneously insert a 6Fr vascular introducer into the vessel with the help of a guidewire (Figure 3B).
- Under ultrasound guidance, place the tip of the introducer 2-3 cm from the bifurcation of the epigastric vein and preterminal valve (for GSV treatment) (Figure 3C) or 2-4 cm below the saphenous-popliteal junction (for SSV treatment).
- Draw 1 mL of NBCA+MS surgical glue in one syringe for veins with a diameter between 8-10 mm, or 2 mL of NBCA+MS surgical glue for veins over 10 mm.
- Draw 7-10 mL of 5% dextrose solution into one syringe.
- Connect the two syringes to the stopcock of the washing catheter of the introducer (Figure 3D).
- Injection time (Figure 4)
- Compress the leg with the ultrasound probe at the level of the bifurcation immediately downstream of the bifurcation itself to stop the blood flow in the saphenous vein (Figure 4A).
NOTE: Compression with the ultrasound probe must be strong and maintained throughout the procedure. - Flush the dead volume of the introducer with dextrose solution (about 2 mL).
- Close the dextrose solution inlet through the stopcock and inject 1 mL of NBCA+MS surgical glue (Figure 4B).
- Through the stopcock, close the NBCA+MS surgical glue inlet and inject the dextrose solution to push the NBCA+MS surgical glue into the vein (Figure 4C).
- At the same time, retract the introducer until it is removed (Figure 4C) to perform a retrograde release of the liquid, adhesive, occlusive, and sclerosing agent (NBCA+MS). Perform a 10 cm occlusion for the GSV or a 7-10 cm occlusion for the SSV.
- Compress the leg with the ultrasound probe at the level of the bifurcation immediately downstream of the bifurcation itself to stop the blood flow in the saphenous vein (Figure 4A).
- Closure time (Figure 5)
- Immediately perform manual compression with the palm, starting from the insertion site and along the course of the vein for 3-5 min. At the same time, always keep the compression with the ultrasound probe at the level of the junction (Figure 5).
- Conclusive time
- At the end of the compression, raise the hand and verify that there is no bleeding from the insertion site.
- Perform an ECD (step 2.3) to check that there is no more blood flow in the saphenous vein (GSV/SSV).
- Under ultrasound guidance, occlude the varicose collateral veins by direct puncture with polidocanol foam, according to the normal and consolidated clinical practice for this treatment13,14.
- Perform an eccentric compression of the saphenous axis with latex strips or rolls of gauze, wrapping the leg from the groin to the knee.
- With the patient still in the clinostatic position, apply a Class II compression stocking (28-30 mmHg) with an open toe, fitting it like a normal pantyhose.
- At the end of the procedure, mobilize the patient immediately, making him take a few steps over a distance of 10-15 m.
- Before discharge, after 2 h, perform an ECD check.
- Discharge the patient with pain relief/anti-inflammatory therapy as needed (i.e., 200 mg of Ibuprofen, one to three times a day).
- Recommend the patient to wear the compression stocking day and night for 10 days, then only during the day for another 30 days.
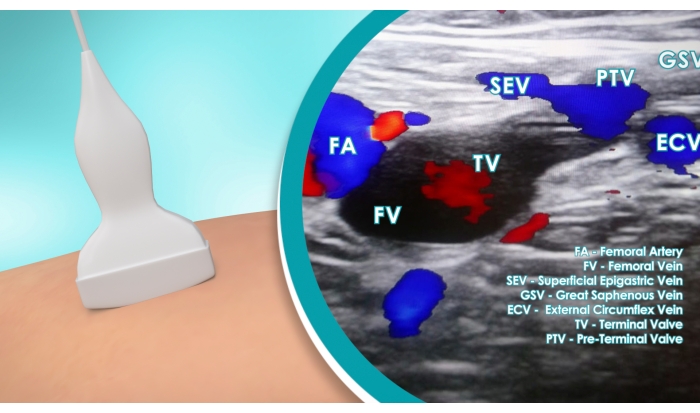
Figure 2: Vascular study. ECD identification of the junction between the epigastric vein and the preterminal valve for the treatment of the GSV. The magnification highlights the ECD image showing the femoral artery (FA), femoral vein (FV), superficial epigastric vein (SEV), great saphenous vein (GSV), external circumflex vein (ECV), terminal valve (TV), and preterminal valve (PTV). Please click here to view a larger version of this figure.
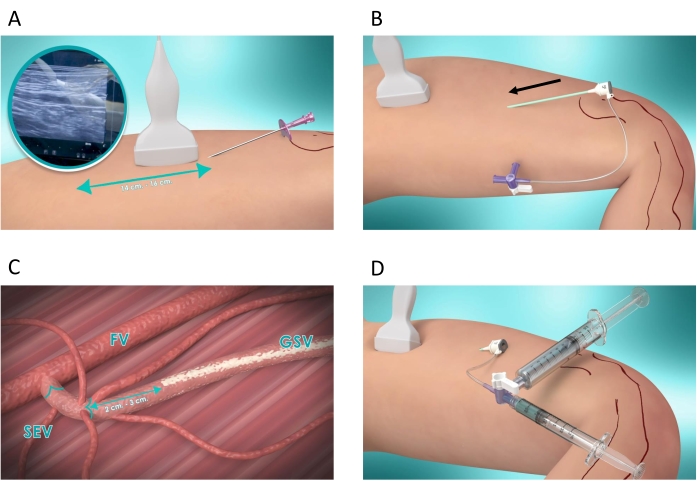
Figure 3: Operative steps. (A) Ultrasound-guided catheterization of the saphenous vein (GSV/SSV) according to the Seldinger technique: a needle is percutaneously inserted 14-16 cm below the junction. Subsequently, a guidewire is inserted through the needle, which is then removed (not shown in the figure). (B) A 6Fr vascular introducer is inserted with the help of the guidewire. At this point, the guidewire is removed and the introducer is left in position (C) Under ultrasound guidance, the introducer tip is positioned 2-3 cm from the bifurcation of the epigastric vein and the preterminal valve (for GSV treatment). The femoral vein (FV), superficial epigastric vein (SEV), and great saphenous vein (GSV) are highlighted in the picture (D) One syringe loaded with 1 mL of NBCA+MS surgical glue and one syringe loaded with 7 mL of 5% dextrose solution are connected to the stopcock of the introducer washing catheter. Please click here to view a larger version of this figure.
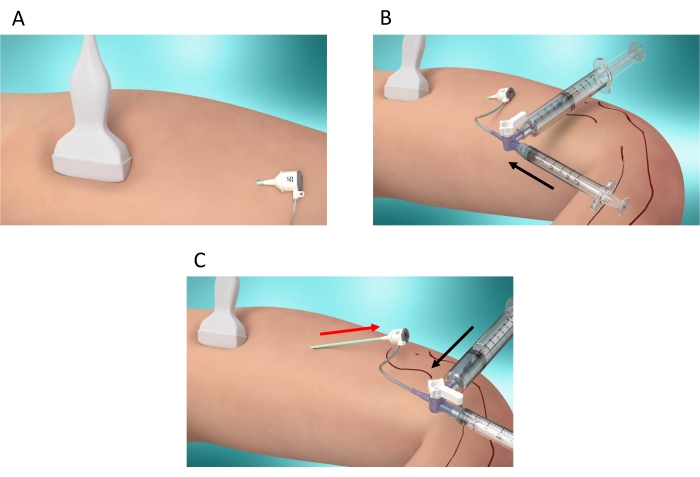
Figure 4: Injection steps. (A) Compression of the leg using the ultrasound probe at the level of the bifurcation immediately downstream of it to stop the blood flow in the saphenous vein (GSV/SSV). (B) Closure of the 5% dextrose solution inlet and injection of 1 mL of NBCA+MS surgical glue (black arrow) (C) Closure of the NBCA+MS surgical glue inlet and injection of the 5% dextrose solution to inject the NBCA+MS surgical glue into the vein (black arrow). At the same time, the introducer is retracted to perform a retrograde injection of the NBCA+MS (red arrow). Please click here to view a larger version of this figure.

Figure 5: Closure time. After removal of the introducer, 5 min of manual compression with the palm of the hand is performed at the level of the insertion site and along the course of the vein. Compression with the ultrasound probe is maintained at the level of the bifurcation during the 5 min manual compression. Please click here to view a larger version of this figure.
