Learning curve
The learning curve for this model is displayed in Figure 6. A progressive decrease in the operating time is observed, reaching approximately 60 min of surgery after 4 weeks of intensive training (Figure 6A). The 5-day postoperative survival also improved with time, reaching 77% during regular practice (Figure 6B). The most frequent causes of mortality were anastomotic leaks and an afferent loop syndrome resulting in biliary peritonitis. We observed no death later in the first month with the technique described in this manuscript. Of note, previous experiments performed without anchoring surgical clips with running sutures led to clip migration in two-thirds of the cases, resulting in one death by small bowel occlusion at 31 days. These results emphasize that mastering this model requires intensive training.
General parameters
Mice with a C57BL6/J background were randomly assigned to the SADI-S group (n = 9; 5 males, 4 females) and the sham control group (n = 4; 2 males, 2 females). Between the SADI-S mice and the sham mice, the mean pre-operative weight (27.9 g ± 0.98 g vs. 28.5 g ± 2.4 g) and age (14.8 weeks ± 7.2 weeks vs. 18.7 weeks ± 10.3 weeks) were not significantly different. One mouse died after SADI-S at postoperative day 4 from an anastomotic leak and was therefore excluded from the following analysis. SADI-S mice experienced significant weight loss in comparison with the sham control mice from the fourth postoperative day: 21.7 g ± 1.6 g versus 29.0 g ± 0.7 g (p = 0.0081) (Figure 7A). Daily food intake (14 days) significantly increased in SADI-S mice (4.4 g ± 0.1 vs. 2.9 g ± 0.6 g per day, p = 0.027) (Figure 7B).
Mice were sacrificed 28 days after surgery. One mouse in the SADI-S group, which did not display significant weight loss, appeared to have duodenal repermeabilization. No such event was observed in the other 7 mice. As displayed in Figure 7C, the hemoglobin concentration was not significantly different from the sham control mice in the SADI-S group after iron supplementation.
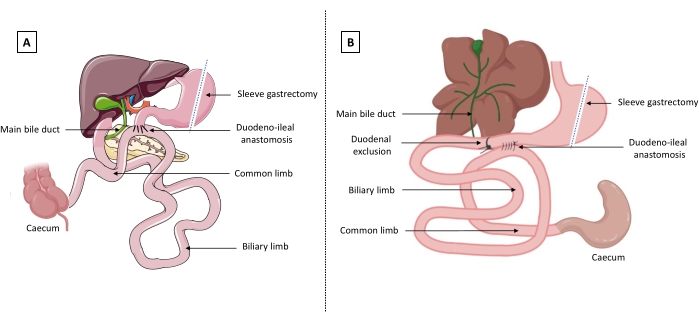
Figure 1: Representation of single anastomosis duodeno-ileal bypass with sleeve gastrectomy (SADI-S). (A) In humans, the duodenum is cut proximally from the main bile duct. A latero-terminal duodeno-ileal anastomosis is performed with the remnant duodenum, defining a biliary limb (before the anastomosis) and a common limb which measures one-third of the total length of the small bowel (after the anastomosis). (B) In mice, the duodenum is excluded by ligature proximally to the main bile duct, and a latero-lateral duodeno-ileal anastomosis is performed. The figure was created with BioRender.com and Servier Medical Art templates which are licensed under a Creative Commons Attribution 3.0 Unported License; https://smart.servier.com/. Please click here to view a larger version of this figure.
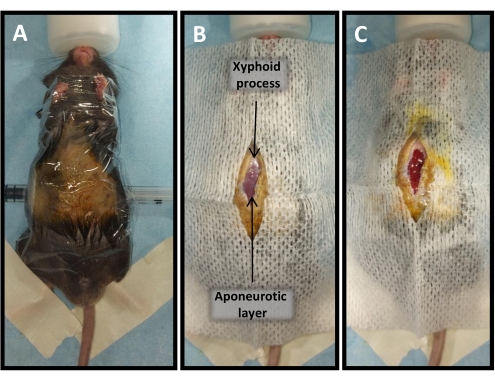
Figure 2: Mouse installation for SADI-S. (A) General installation. (B) Skin opening from the xyphoid process (sternal base) to the middle of the abdomen. (C) Musculo-aponeurotic layer and peritoneal opening. Please click here to view a larger version of this figure.
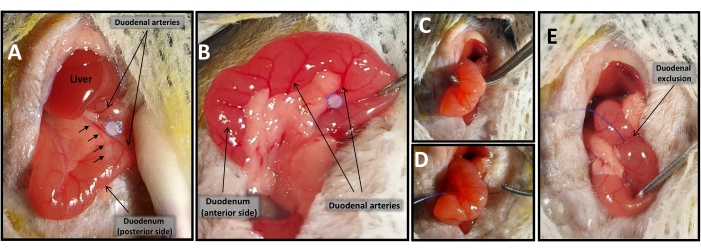
Figure 3: Duodenal exclusion. (A) Avascular window between duodenal arteries (blue dotted circle) on the posterior side of the duodenum, localized before the main bile duct (black arrows). (B) Avascular window between duodenal arteries (blue dotted circle) on the anterior side of the duodenum. (C,D) Duodenal exclusion using 6-0 non-absorbable suture. (E) Final view of excluded duodenum. Please click here to view a larger version of this figure.
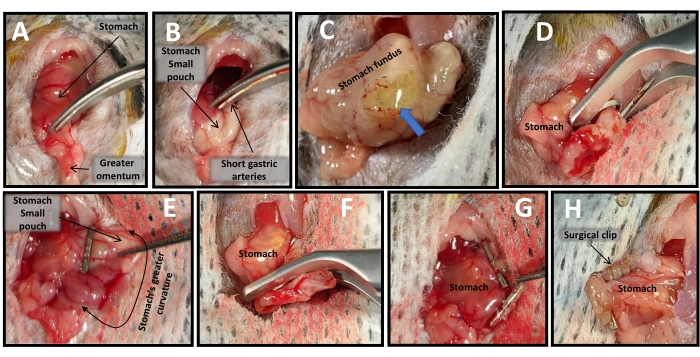
Figure 4: Sleeve gastrectomy. (A) Greater omentum removal. (B) Incision of short gastric arteries. (C) Initial gastrotomy (blue arrow). (D–G) Stomach cardiac region removal using two surgical clips. (H) Surgical clips anchoring using 6-0 non-absorbable suture. Please click here to view a larger version of this figure.
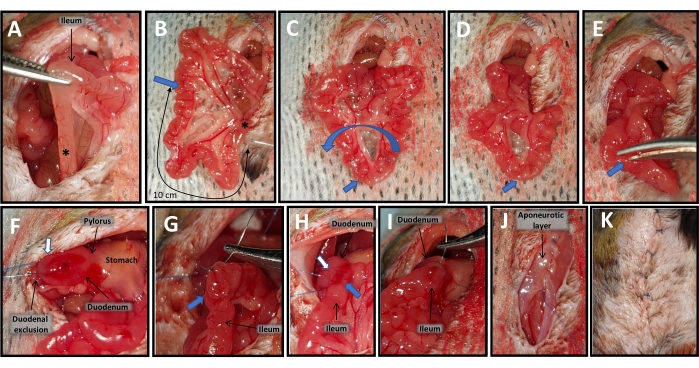
Figure 5: Duodeno-ileal anastomosis. (A) Identification of the last ileal loop (asterisk). (B) Count 10 cm (one-third of the total length of the small bowel) from the last ileal loop (asterisk) to the site of the future anastomosis (blue arrow). (C,D) Small bowel rotation around the site of the future anastomosis (blue arrow). (E) Ileal enterotomy. (F) Duodenotomy (white arrow). (G–I) Side-to-side anastomosis in two layers between the duodenotomy (white arrow) and the ileal enterotomy (blue arrow). (J) Musculo-aponeurotic layer closure. (K) Skin closure. Please click here to view a larger version of this figure.
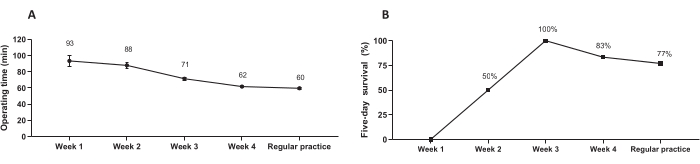
Figure 6: The SADI-S procedure learning curve. (A) The effect of training on the duration of the operation. Data are presented as the mean value ± SEM. (B) The effect of training on five-day survival. Data are presented as percentages. Please click here to view a larger version of this figure.
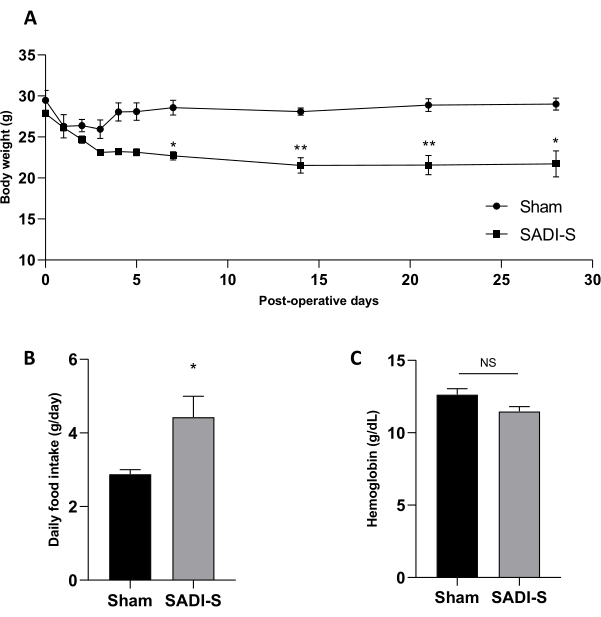
Figure 7: General parameters after SADI-S. (A) Postoperative body weight, (B) food intake measured for 24 h at day 14, and (C) blood hemoglobin concentrations were compared between SADI-S and sham control mice. Data are presented as the mean ± SEM. Statistical comparisons were made with two-way ANOVA (with Sidak's multiple comparisons test) or Mann-Whitney non-parametric tests. * p < 0.05; ** p < 0.01. Please click here to view a larger version of this figure.
