ELST are rare and locally aggressive neoplasms that arise on the posteromedial surface of the temporal bone. Due to their slow growth rate, and the initial paucity of the symptoms, the diagnosis is often delayed, resulting in an advanced tumor stage. Since the surgery morbidity as well as the oncologic outcomes are strongly correlated with the tumor dimensions and extension6,8,13,15, an early diagnosis is necessary.
The first step for a prompt diagnosis is the clinical evaluation of patients. The medical and familiar history of a patient that may refer to the presence of a VHL has to be thoroughly investigated. Anyway, in the case reported herein, no history of known VHL was reported from the patient, as well as previous suggestive symptoms.
Further, since hearing loss and vertigo are a frequent association of symptoms underlying a number of peripheric clinical conditions of the ear, ranging from hydropic diseases of the inner ear to the acute unilateral vestibulopathy, but also central disturbances, is important to rule out neurological and neuroradiologic examinations in every patient reporting Meniere-like symptoms. In fact, even when the clinical picture seems to indicate a pure peripheric lesion, an imaging study of the brain, the brainstem, and the petrous bones should be always advised, even to exclude central diseases leading to peripheric deficit, but, mainly, for the study of IAC and the PCA. Those aspects are even more important when a patient presents a confirmed diagnosis of VHL or occurrences compatible with such a disease.
In the case herein reported, the diagnosis was appropriately suspected based on a rapid imaging study after the symptom’s onset and intraoperatively confirmed shortly afterward. As shown here, an early diagnosis based on the clinical signs and symptoms and prompt imaging studies can lead to a more sustainable surgery, with low risk of postoperative residuals or recurrence of disease.
Even if hearing loss and vertigo are a frequent association of symptoms underlying many peripheric clinical conditions of the ear, neuroradiologic examination have to be promptly ruled out to exclude misdiagnosed central disturbances, as well as IAC or PCA diseases. Furthermore, an accurate anamnesis should investigate for occurrences that are compatible with VHL, such as prior diagnosis of tumors such as pheochromocytoma, cerebellar hemangioblastoma, or retinal angioma; prior comparison of cysts at kidneys, liver, pancreas, or genital tract; and symptoms like headache, asthenia, hypertension, ataxia, or vision disturbances14.
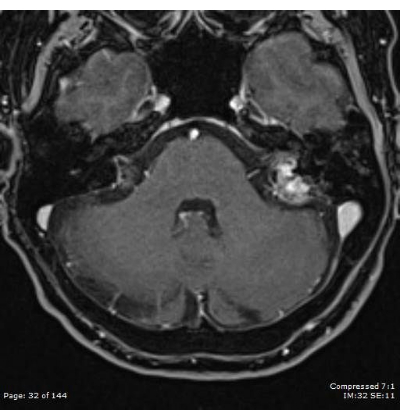
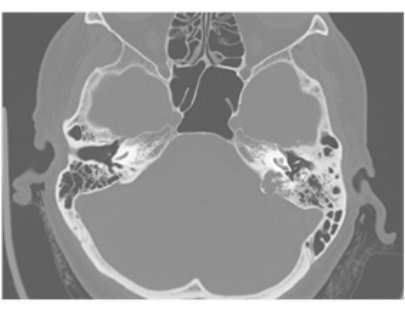
In our third level referral hospital, all the patients reporting cochlear or vestibular symptoms promptly undergo an imaging study, preferably a high-field MRI study of the brain and the brainstem and the petrous bone with contrast agent, for an accurate evaluation of those structures, the IAC and the PCA, and a HRCT scan study, for the evaluation of the bony structures of the petrous bone, if needed. The occurrence of a mass arising from the posterior face of the petrous bone, especially if associated with a suspected or known diagnosis of VHL, is highly suggestive of ELST.
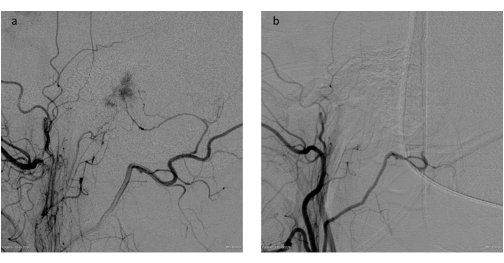
Before the surgical resection of such a mass, the principal decisions to be made from the clinicians are the execution of a preliminary embolization of the tumor and the surgical access to the lesion. There is no global consensus on the necessity of a preliminary embolization6,8,15, especially in low-staging masses, but this procedure may lead to a reduction in the bleeding of the mass during the resection, ensuring a cleaner surgical field and so an easier removal of the mass.
In this protocol for the managing of ELST, preoperative embolization is always proposed, even for limited and low-staging masses, since it leads to reduced surgery time, reduced blood loss, easier surgery and therefore, reduced morbidity.
The early diagnosis, based on an accurate and prompt clinical assessment and imaging study in patients reporting Meniere-like symptoms, can guarantee an early-stage surgery in case of an ELST. Further, thanks to a low staging of disease at the diagnosis, an accurate embolization and a precise surgical resection of the mass, it is usually possible to achieve good oncologic results, without disease recurrence and long disease-free survival period, avoiding or reducing the incidence of the main complications of major petrous bone surgery, such as the facial nerve palsy or the postoperative CSF leaks.
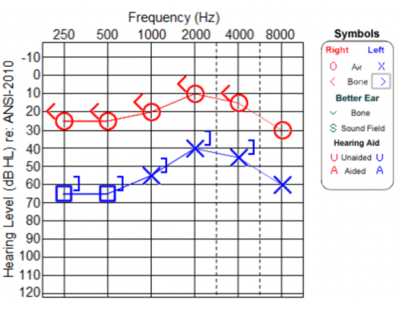
In the presence of an ELST, the imaging assessment, which should include an MRI and an HRCT study, make it possible to stage the tumor. According to the stage of the tumor and the audiologic assessment of the patient, it is possible to define a surgical approach and estimate a prognosis15.
To date, in fact, surgical resection is considered the treatment of choice in patients with an ELST. Another therapeutic option is the radiation therapy8,15. However, since the role of adjuvant radiation therapy is not well reported yet8,16, it should be considered for patients with residual disease after surgical resection, or in inoperable patients due to morbidity or the excessive tumor extension8,10,15.
As reported by Nelson and colleagues15, another therapy for inoperable patients could be represented by pazopanib, a multikinase inhibitor and antiangiogenic agent. Anyway, there is no evidence currently supporting the use of this drug as primary or adjuvant therapy for ELSTs.
Before the surgical resection, clinicians can propose a preliminary embolization of the mass. Even if recommended by some authors6,8, especially in situations where vascularity of the tumor could otherwise preclude a complete resection, ELST preoperative embolization is not constantly reported in literature13. Even for small masses, in accordance with other authors (e.g., Wu and colleagues6), an accurate preoperative embolization is always ruled out in our center, since it can reduce the difficulty and the morbidity of the surgery, in addition to the risk of severe intraoperative blood loss. In fact, since the main goal in the treatment of ELST is full surgical eradication8,15, small masses must be treated with reduced bleeding as one of the key points in managing this pathology.
As reported, a low-staging mass with controlled bleeding can be removed through an exclusive posterior labyrinthectomy approach, guaranteeing little postsurgical morbidity and good oncologic results. After the surgical removal of the mass, clinicians must initially deal with the postoperative symptoms and monitor the patient for complications. The eventual specific complications of such a major surgery on the petrous bone include CSF leakages and facial nerve palsy.
According to the literature, postsurgical complications, as far as residual disease after resection are, comprehensibly, more frequent when the tumors are extensive and their resection requires a highly invasive surgery6,8,15. In the case described herein, no major postsurgical complications, as well as no residual disease, were reported. Further, after the histologic confirmation of an ELST, patients with such a tumor should exclude the coexistence of a VHL through specific genetic studies. Genetic studies excluded VHL for the patient herein discussed.
In a recent systematic review by Tang and colleagues8, from the analysis of a total of 253 unique tumors in 247 patients, reported recurrence or progression after surgery was 21.8%, after a mean time of 46.7 months (from 3 to 180 months) and the disease-free survival was 47.6 ± 46.4 months in patients with sporadic disease and 49.8 ± 48.3 months in patients with VHL-associated disease.
Even if there is no consensus on the follow-up of the patients after the resection of an ELST, an MRI study every 6 to 8 months could effectively identify a recurrence or a progression of the disease after surgery. It is not clear how long the MRI follow-up should be. In their systematic review, Tang and colleagues reported a recurrence even after 15 years from surgery, while Poletti et al.10 and Sykopetrites15 reported cases with recurrence after more than 10 years. Thus, a very lasting and accurate protocol of follow up should be considered based on the possibility of a recurrence of the disease after such a long period.
In conclusion, the case reported herein demonstrates the importance of managing ELST through early diagnosis based on an accurate clinical and radiological assessment. Further, an eventual preventive embolization of the mass and an accurate surgery on a small, low-grade tumor, can lead to good oncologic results with limited postoperative surgical morbidity. Despite this, a long-lasting MRI follow up should be always advised, since recurrence of the disease is possible even after a long time after surgery.