PG-induced model mice developed symptoms of peripheral arthritis, characterized by redness and swelling of the extremities and toes, and gradually developed axial arthritis as early as week 14, which is very similar to the manifestation of AS. Therefore, the AS mouse model was considered successful if the arthritis index (AI) was over 3 points at 14 weeks after the last injection22. When the paws of the mice appeared swollen, the Du-moxibustion treatment was carried out once a week for a total of 3x. After treatment, the mice were euthanized by cervical dislocation under isoflurane deep anesthesia, their blood was collected, and the ankles were excised.
Effects of Du-moxibustion on motor coodination and autonomic movement
Bovine PG-induced AS was adopted as a model to observe the effect of Du-moxibustion at the Du meridian on motor coordination. Initially, the joint swelling score was used to assess whether the model was successful, and motor coordination and autonomic movement were evaluated using the rotarod test and OFT.
Evaluation of AI determined the severity of peripheral arthritis. After modeling, two-way repeated-measures ANOVA revealed that the joint swelling scores in the model and Du-moxibustion groups significantly increased compared with those in the control group before the Du-moxibustion (P < 0.01; Figure 6A). Du-moxibustion treatment decreased joint swelling scores compared with those of the model group after the Du-moxibustion (P < 0.05; Figure 6A).
The rotarod test was employed to evaluate motor coordination and balance. Two-way repeated-measures ANOVA revealed significant differences over time (F = 13.928, P = 0.000 < 0.05) and interaction effects of time and group (F = 12.583, P = 0.000 < 0.05). After modeling, the latency time of the control group was not different from that before modeling. However, after modeling, the latency times of the model and Du-moxibustion groups significantly decreased compared with those in the control group (P < 0.01; Figure 6B), and there were no significant differences between the model group and the Du-moxibustion group (P > 0.05; Figure 6B). After treatment, the latency time of the Du-moxibustion group significantly increased compared to that of the model group (P < 0.05; Figure 6B). These results indicated that Du-moxibustion was effective in improving motor coordination in AS mice.
OFT was performed to detect autonomic movement. The parameters were collected and analyzed automatically using the software (Figure 6C–E); the total distance and average speed were mainly observed in this study. There was no significant difference in the total distance and average speed among the groups before modeling (P > 0.05; Figure 6C,D). After modeling, the total distance and average speed significantly reduced compared with the control group (P < 0.05; Figure 6C,D). After treatment, the total distance and average speed of the Du-moxibustion group significantly increased compared to those of the model group (P < 0.05; Figure 6C,D). These results indicated that Du-moxibustion was effective in improving autonomic movement in AS mice.
Effects of Du-moxibustion on ankle joint pathology
HE staining was used to observe the pathological changes in the ankle joint. In the control group, there was no damage to the synovium structure, no congestion in the synovium, and no obvious inflammatory cell infiltration and necrosis. However, in the model group, synovium hyperplasia and infiltration were observed in the joint cavity, in addition to inflammatory cell infiltration and tissue edema. Combined with AI evaluation, it was proved that the AS model was successfully established. Compared with the model group, the synovium of mice in the Du-moxibustion group was more intact, interstitial edema was reduced, and the articular cartilage was relatively intact (Figure 7).
Effects of Du-moxibustion on plasma IL-17 and TNF-α levels
ELISA was performed to measure IL-17 and TNF-α in the plasma. The plasma IL-17 and TNF-α levels of the model group were significantly increased compared with those of the control group (P < 0.01; Figure 6F,G). Du-moxibustion decreased plasma IL-17 and TNF-α levels (P < 0.05; Figure 6F,G).
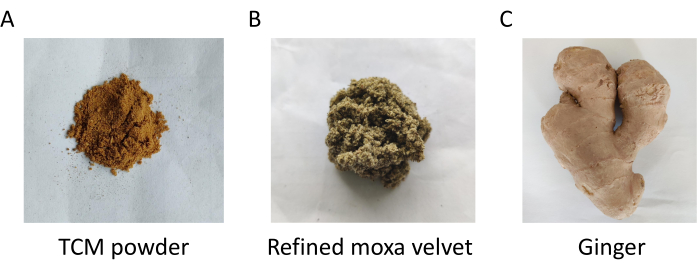
Figure 1: The raw materials needed for Du-moxibustion. Please click here to view a larger version of this figure.
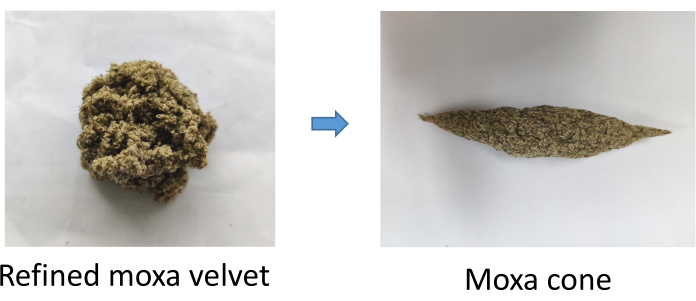
Figure 2: Making a moxa cone. Please click here to view a larger version of this figure.

Figure 3: Prepare ginger water and make a trapezoidal ginger column. Please click here to view a larger version of this figure.
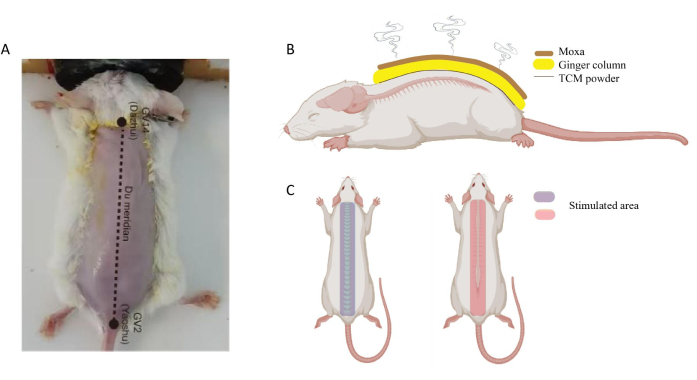
Figure 4: Location of GV14 and GV2 in mouse. (A) GV14 located at the subspinous process of the seventh cervical vertebra; GV2 located in the hiatus sacral canal. (B) Schematic diagram of Du moxibustion on the mouse. (C) Stimulated area of Du moxibustion. Please click here to view a larger version of this figure.
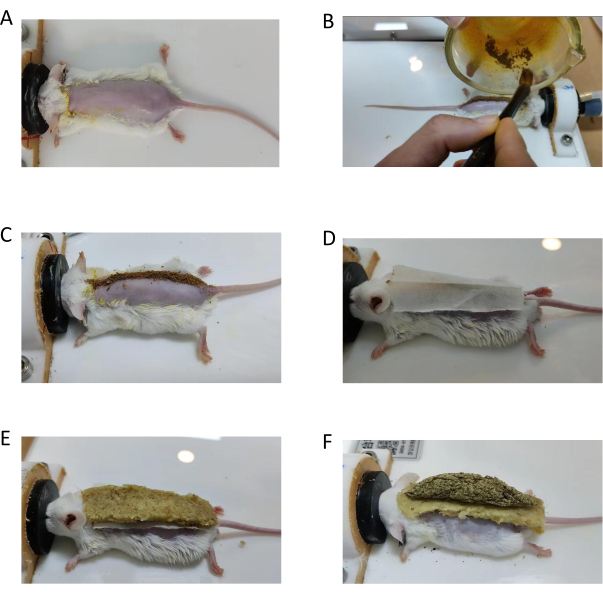
Figure 5: Operation procedure of Du-moxibustion in mouse. (A) Shave the hair and smear the ginger juice on the mouse in the prone position. (B,C) Sprinkle TCM powder evenly. (D) Cover the powder with mulberry paper. (E) Fix the ginger column on the mulberry paper firmly. (F) Put a moxa cone on the ginger column; then, light it. Please click here to view a larger version of this figure.
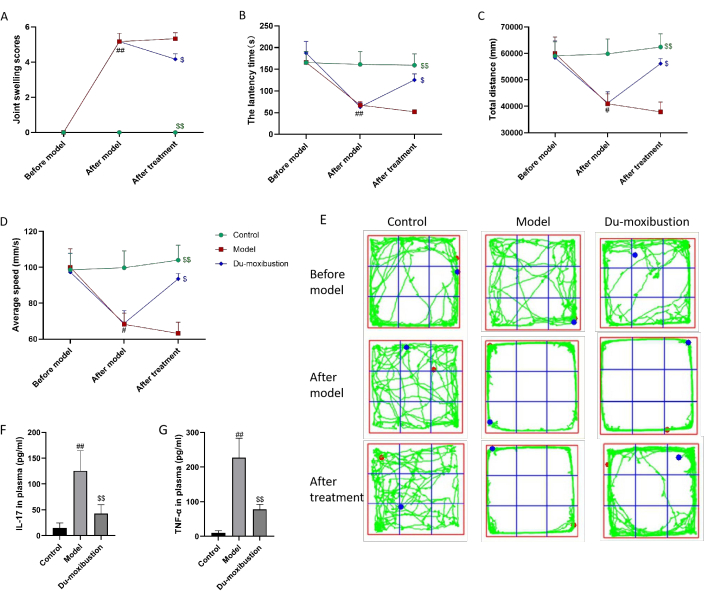
Figure 6: Effects of Du-moxibustion on motor coordination, autonomic movement, and IL-17 and TNF-α levels. (A) The joint swelling scores in mice. (B) The latency time in the rotarod test. (C–E) Total distance, average speed, and track diagram of OFT. (F) IL-17 levels in plasma. (G) TNF-α levels in plasma. Values are expressed as the mean ± SEM (n = 6). ##P < 0.01, #P < 0.05 versus the control group; $$P < 0.01, $P < 0.05 versus the model group. Abbreviations: IL = interleukin; TNF = tumor necrosis factor; OFT = open field test. Please click here to view a larger version of this figure.
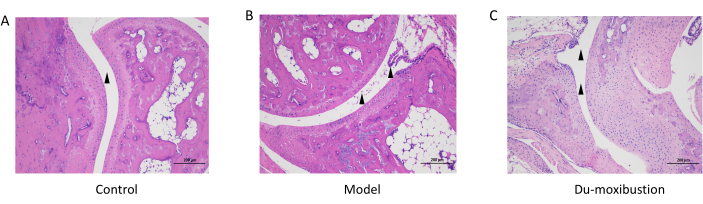
Figure 7: HE staining of the ankle joint. (A) The joint cavity was smooth without inflammatory infiltration in the control group. (B) In the model group, synovium hyperplasia and infiltration were observed in the joint cavity. (C) In Du-moxibustion group, the joint cavity of mice was smooth and edema was alleviated. Scale bars = 200 µm. Abbreviation: HE = hematoxylin-eosin. Please click here to view a larger version of this figure.
