Sonographically normal exam
Normal kidney ultrasound
The echogenicity of the kidney capsule and limited anatomic variability (except for the occasional pelvic kidney or the even more rare horseshoe kidney) allow for easy identification of the kidneys with bedside POCUS. The kidneys will have a typical bean-shaped appearance, measuring on average 9-13 cm, though size varies with patient height and weight (Figure 2, Video 1). The outer cortex is typically hypoechoic relative to the adjacent spleen and liver. Interior to the cortex is the kidney medulla, which is comprised of anechoic pyramids with cortical tissue extending into the medulla and separating the pyramids. The renal sinus is comprised of the renal pelvis, collecting system, sinus fat, vessels, and lymphatics. The sinus fat contributes to the hyperechoic appearance of this region of the kidney (Figure 9). The transverse or short axis of the kidney, as seen by rotating the probe 90 degrees, is characterized by the mid-portion of the kidney appearing as a C-shaped pattern with the localization of renal vessels and ureter (Figure 5, Figure 10, and Video 2, Video 3, and Video 4).
Normal bladder ultrasound
Whenever feasible, the bladder should be visualized in both the transverse and sagittal planes. The transverse view is obtained with the probe indicator pointing towards the patient's right side and normally shows the bladder in a circular cross-section (Figure 7, left). The sagittal bladder view is obtained with the probe indicator pointing cranially, and it normally shows the bladder as an irregular structure with a broad portion caudally and a narrow portion cranially (Figure 7, right). As the bladder distends, the sagittal view will tend to show a bladder shape that is increasingly circular/ovoid.
Key abnormal findings
Key abnormal kidney findings
Identification of kidney abnormalities with bedside ultrasound can provide critical clues to a patient's pathology and causes of kidney dysfunction. Assessment of kidney size, presence and degree of hydronephrosis, and identification of stones, cysts, and masses are the predominant objectives of bedside ultrasound.
Assessment of kidney size
Measurement of kidney length may help distinguish AKI from chronic kidney disease (CKD) or acute-on-chronic kidney injury as kidney size is expected to decrease with decreases in kidney function15. Normal kidney size is 9-13 cm in its longest dimension, 3-7 cm wide (in the coronal plane) and 3-6 cm thick (in the transverse plane)16. Also, as kidney size varies within the adult population, differences in size between the left and right kidneys can suggest differential kidney function between them. The kidney cortex is also known to decrease in size in the setting of CKD from its normal thickness of 7-10 mm as well as become more echogenic17 (Video 5). Certain kidney pathologies may also be associated with an increase in kidney size. Inflammatory states (such as AIN or glomerulonephritis) and infiltrative processes may be associated with an increase in kidney size.
Hydronephrosis
An obstructive process that leads to a dilated renal pelvis and calyces is termed hydronephrosis. In contrast, the term pelvicaliectasis is used when the renal pelvis and calyces are dilated without any evidence of obstruction. POCUS is frequently used to assess hydronephrosis as an indicator of obstruction. Obstruction may be due to a stone distal to the kidney, such as ureteropelvic junction, ureter, or ureterovesical junction. Additionally, a bladder mass obstructing a ureterovesical junction or urethral orifice (Figure 11), a prostatic mass, or hypertrophy can lead to hydronephrosis. Finally, extrinsic compression from a mass or lymphadenopathy is another potential cause. Hydronephrosis of the kidneys, independent of the cause, has a similar ultrasonographic appearance. However, one should note if hydronephrosis is unilateral or bilateral, as this will support or refute certain diagnoses.
As noted above, normal kidney parenchyma includes fat, which gives it a hyperechoic appearance. The obstructed urinary tract results in a distended collecting system, changing the ultrasonographic appearance of the kidney from hyperechoic to hypoechoic and sometimes anechoic. As the severity of hydronephrosis increases, the appearance becomes more anechoic, extending proximally to the kidney cortex. Hydronephrosis is graded as being either mild, moderate, or severe. Mild hydronephrosis is characterized by dilation of the renal pelvis and the calyces (Figure 12A, Video 6). As hydronephrosis progresses to moderate, the tips of the renal pyramids flatten and become concave due to increasing urine volume and pressure (Figure 12B,C, Video 7). In cases of severe hydronephrosis, the renal pelvis and calyces undergo further dilation, while the cortex begins to get thinner, resulting in a frequently described bear claw appearance (Figure 12D and Figure 13, Video 8). Further, an important false positive for hydronephrosis is a common normal variant termed extra-renal pelvis18. This describes the finding of a renal pelvis located outside the kidney itself and may be present in as much as 10% of the population18. The calyces in cases of an extra-renal pelvis are not sonographically visible, in contrast to the readily visible calyces in hydronephrosis due to their dilatation (Figure 14, Video 9).
Kidney cysts
Kidney cysts, both sporadic and inherited, are commonly seen on POCUS and characterized as simple or complex. Simple cysts are observed as round or oval, well-defined, thin-walled structures exhibiting acoustic enhancement on the distal wall (enhanced echogenicity attributed to increased echoes). CT imaging (Figure 15, Video 10, Video 11) uses the Bosniak criteria for the classification of cysts. While the validation of the Bosniak criteria in ultrasound imaging is not as extensive, they are commonly employed to categorize patients into two groups: those requiring follow-up imaging and those who do not. Any cyst that fails to meet the following criteria: being oval/circular, having a thin wall without septations, and lacking posterior acoustic enhancement on the far wall, should undergo further imaging evaluation19–22. If multiple cysts are observed bilaterally, one should consider the possibility of polycystic kidney disease or acquired cystic kidney disease23.
Kidney masses
As noted above, abnormalities seen on kidney ultrasound that are not consistent with a simple cyst should receive further radiographic evaluation. The prevailing malignancy is renal cell carcinoma, distinguished by a partially cystic mass with heterogeneous features (Figure 16, Video 12, and Video 13). Benign kidney masses most commonly are angiomyolipomas and oncocytomas24.
Key abnormal bladder findings
In the evaluation of oliguria/anuria and/or AKI, bladder and kidney POCUS can aid in narrowing the differential diagnosis (Figure 17). The initial step, outlined in the algorithm, is to determine if the patient has an indwelling invasive urinary (Foley) catheter. If a Foley catheter is present, the subsequent examination involves checking for the catheter balloon in the bladder. If the balloon is not visible, it suggests catheter misplacement (e.g., the catheter tip is in the urethra). If the catheter balloon is visible but the bladder is distended (Figure 18), obstruction is likely. If the bladder is small/decompressed (Figure 19), it indicates either complete ureteral obstruction, pre-renal/intrinsic kidney disease, or unilateral obstruction in patients with a solitary kidney. To differentiate, kidney ultrasound is crucial; hydronephrosis significantly raises the probability of ureteral obstruction, while its absence argues against it. Note that this algorithm serves as a heuristic rather than a definitive diagnostic tool, as some cases of low urine output and AKI can coexist, such as a patient with chronic hydronephrosis developing acute pre-renal/intrinsic kidney disease.
In reference to the algorithm in Figure 17, when the patient lacks an indwelling urinary catheter, the sonographic screening for low urine output and/or AKI commences with the qualitative or quantitative evaluation of bladder size. A grossly distended bladder (Figure 20) suggests potential causes such as bladder outlet obstruction (e.g., benign prostatic hyperplasia) or ineffective detrusor muscle action (e.g., spinal or epidural anesthesia). In cases where the bladder is small/decompressed, the differential diagnosis mirrors that of an indwelling urinary catheter with a small/decompressed bladder-either (1) complete ureteral obstruction or (2) pre-renal or intrinsic kidney disease. To distinguish between these possibilities, an assessment of the patient's kidneys for signs of hydronephrosis, as described earlier, is essential.
During the assessment of the bladder for factors contributing to low urine output, it is possible to occasionally observe echodensities within the bladder lumen. For instance, Figure 11 (see also Video 14) illustrates a bladder containing a sizable, irregular echodensity, determined to be a combination of a bladder tumor and blood clots. In practical terms, the use of ultrasound faces challenges in differentiating between masses and blood clots within the bladder. However, both findings are considered grossly abnormal and necessitate further imaging and/or consultation with Urology for guidance on long-term care.
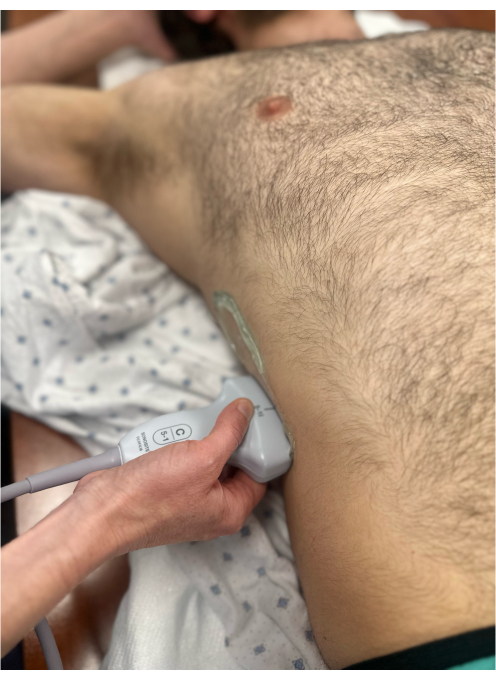
Figure 1: Curvilinear probe to the mid axillary line on the right side to visualize the right kidney in the longitudinal view. The probe marker is pointing to the patient's head and hence is not visible in the image. Please click here to view a larger version of this figure.
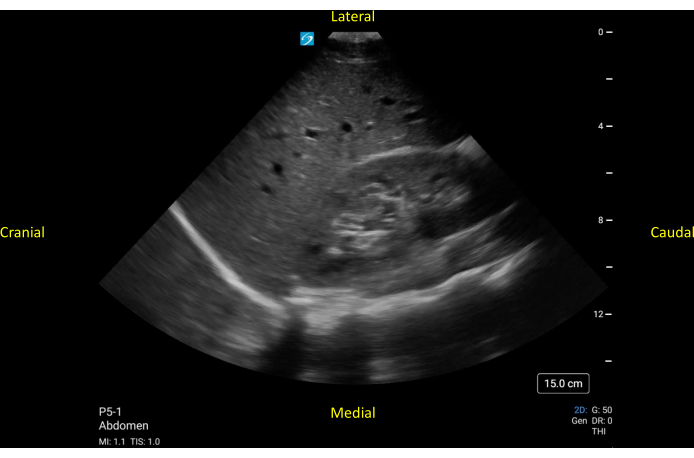
Figure 2: Longitudinal view of a normally functioning right kidney. The cranial to the right kidney, the liver, and the diaphragm are seen. Medial to the kidney, the individual vertebrae are seen. Please click here to view a larger version of this figure.
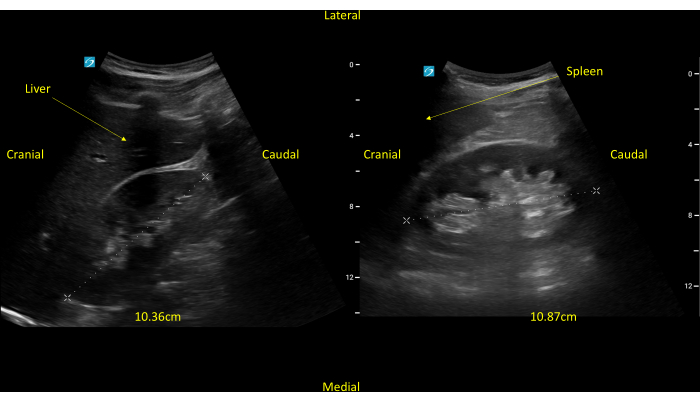
Figure 3: Longitudinal views of both the right and left kidney, respectively. The kidneys measure a little over 10 cm each. Please click here to view a larger version of this figure.

Figure 4: Curvilinear probe to the mid axillary line on the right side to visualize the right kidney in the short axis view. The probe marker is pointing posteriorly and hence, is not visible in the image. Please click here to view a larger version of this figure.
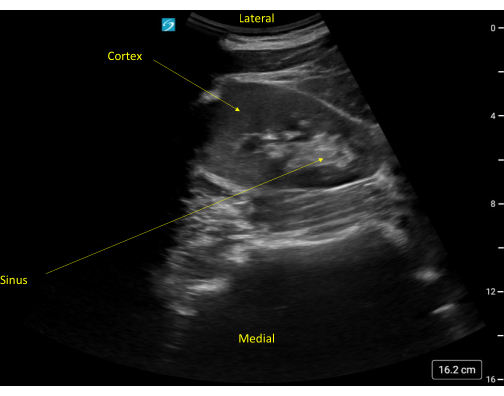
Figure 5: Short axis view of a normal appearing kidney. Note the rib shadow to the right of the kidney. Please click here to view a larger version of this figure.

Figure 6: Curvilinear probe to the suprapubic area to visualize the bladder in the transverse orientation. The probe marker is pointing to the patient's right and, hence, is not visible in the image. Please click here to view a larger version of this figure.
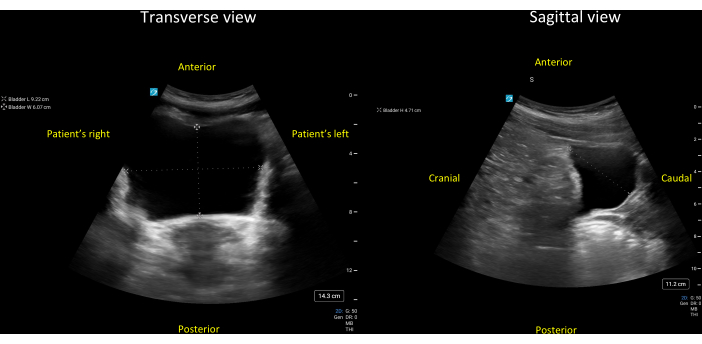
Figure 7: Transverse (left panel) and sagittal (right panel) views of a grossly normal bladder. The three diameters of this bladder have been measured as 9.2 cm (lateral-to-medial), 6.1 cm (anterior-to-posterior), and 4.7 cm (cranial-to-caudal). Entering these three diameters and a correction factor for the triangular bladder of 0.69 (Protocol step 7.3.3.1), one gets the following estimate for the bladder volume = 0.69 * 9.2cm * 6.1cm * 4.7cm = 182cm3 (mL). Please click here to view a larger version of this figure.

Figure 8: Curvilinear probe to the suprapubic area to visualize the bladder in the sagittal orientation. The probe marker is pointing to the patient's head and, hence, is not clearly visible in the image. Please click here to view a larger version of this figure.
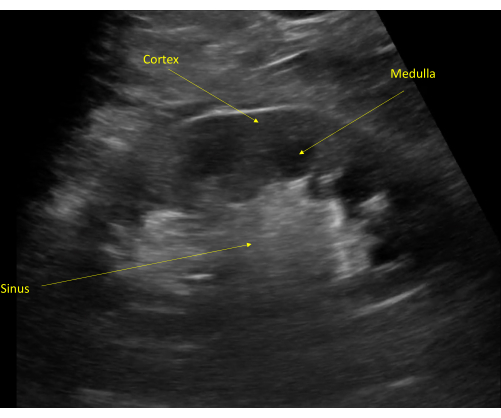
Figure 9: The kidney cortex is typically seen as hypoechoic to the liver (unlabeled, superior to the kidney). The kidney medulla is visible distal to the cortex with visible renal pyramids. The collecting system is seen as a hyperechoic structure due to the renal sinus fat. Please click here to view a larger version of this figure.
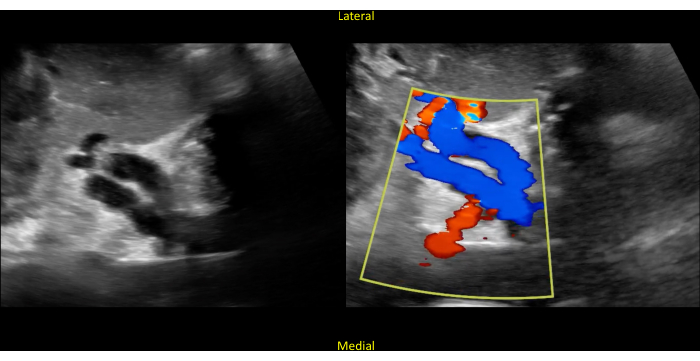
Figure 10: Short axis view of the kidney. The image shows hollow structures in the center (left panel). Color Doppler confirms that these structures represent the renal vasculature (right panel). Blue represents flow away from the probe, and red represents flow towards the probe (remembered by the mnemonic "BART"; blue away, red towards). Please click here to view a larger version of this figure.
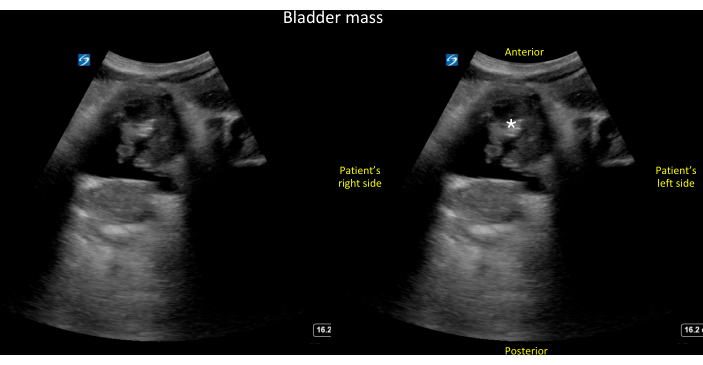
Figure 11: Transverse view of the bladder. Unlabeled (left panel) and labeled (right panel) transverse view of the bladder showing a large, irregular echo density within the bladder lumen that turned out to be a combination of tumor and blood clots (see also Video 14). Please click here to view a larger version of this figure.
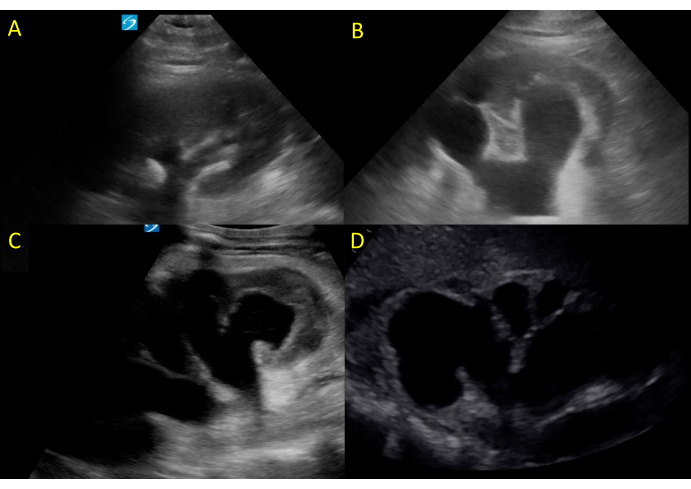
Figure 12: Hydronephrosis of varying degrees. (A) shows mild hydronephrosis, (B,C) moderate hydronephrosis, and (D) severe hydronephrosis. Please click here to view a larger version of this figure.
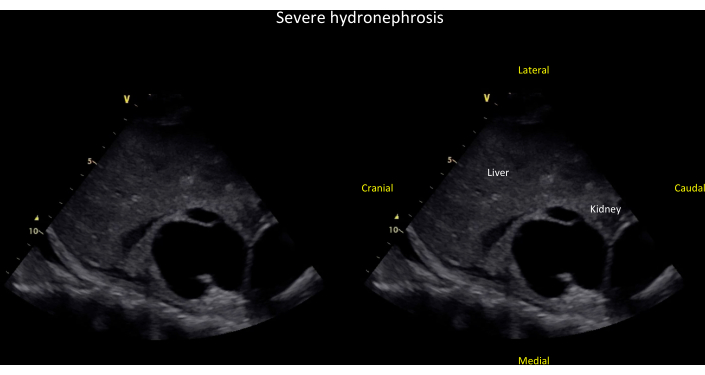
Figure 13: Coronal view of the right kidney showing severe hydronephrosis. Unlabeled (left panel) and labeled (right panel) coronal view of the right kidney showing severe hydronephrosis, defined by dilation of major and minor calyces and cortical thinning (see also Video 8). Please click here to view a larger version of this figure.
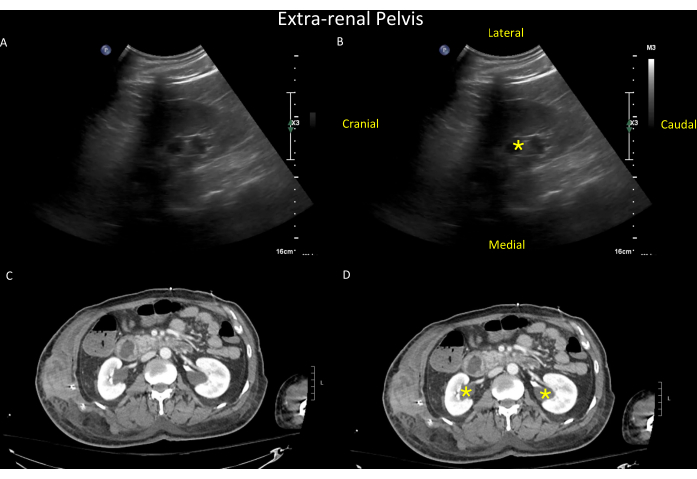
Figure 14: Sonographic findings in the right kidney. Unlabeled (top left, A) and labeled (top right, B) views of the right kidney showing the sonographic findings of an extra-renal pelvis (yellow asterisk). The extra-renal pelvis is a normal variant found in up to 10% of the population, where the renal pelvis lies outside the kidney. Extra-renal pelvis can mimic hydronephrosis except that in hydronephrosis, the calyces are visible and dilated, whereas, in extra-renal pelvis, the calyces are normal-sized and hence not visible. For illustrative purposes, a CT scan of the same patient is shown in the bottom panels (unlabeled in C and labeled in D, with extra-renal pelvis seen bilaterally (yellow asterisk in D) (see also Video 9). Please click here to view a larger version of this figure.
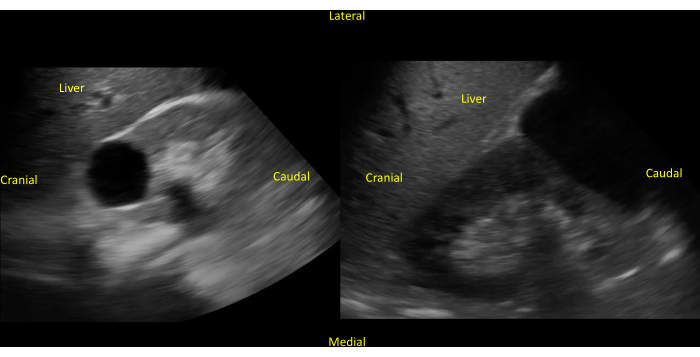
Figure 15: Presence of renal cyst in the right kidney. An unlabeled (left panel) image of a simple renal cyst in the center of the right kidney is viewed on the long axis. Unlabeled (right panel) image of a larger simple renal cyst in the inferior pole of the right kidney. Please click here to view a larger version of this figure.
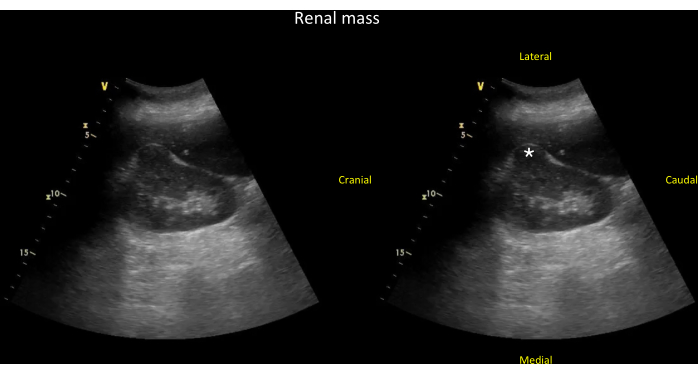
Figure 16: Coronal view of the right kidney showing a kidney mass. Unlabeled (left panel) and labeled (right panel) coronal view of the right kidney showing a kidney mass (*) that is arising from the kidney cortex and has disrupted the expected normal oval shape typically seen in this view (see Video 13). Please click here to view a larger version of this figure.
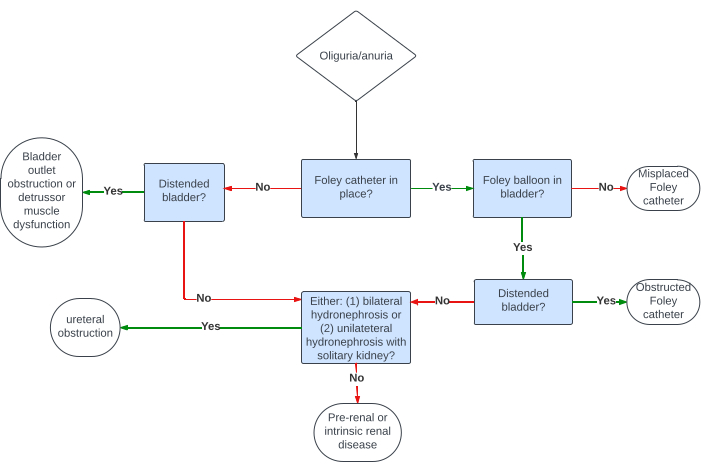
Figure 17: An algorithm showing how the combined bladder and kidney ultrasound can be used to narrow the differential diagnosis of oliguria/anuria. Please click here to view a larger version of this figure.
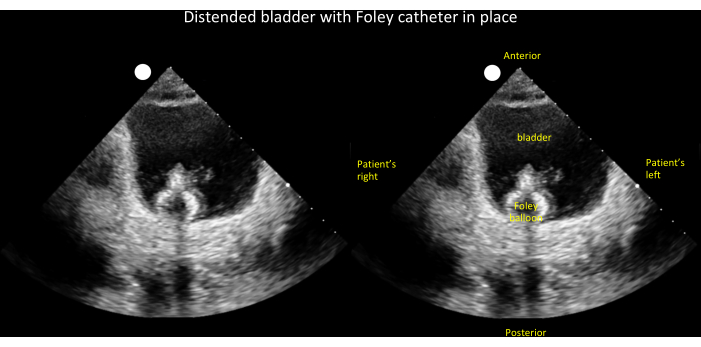
Figure 18: Unlabeled (left panel) and labeled (right panel) transverse view of a distended bladder with Foley balloon visible inside. This finding, when coupled with low urine output, narrows the differential diagnosis of oliguria/anuria to an obstructed Foley catheter (see Figure 17). Please click here to view a larger version of this figure.
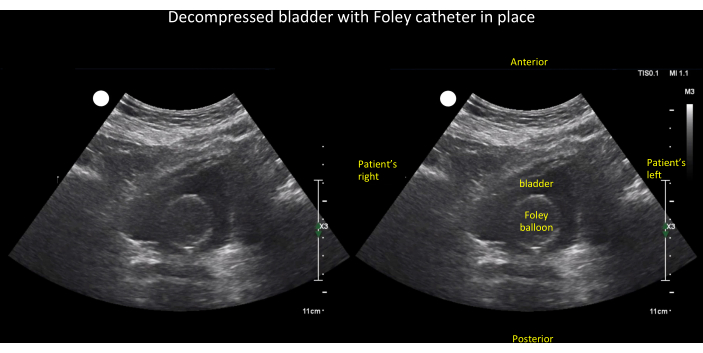
Figure 19: Unlabeled (left panel) and labeled (right panel) transverse view of an empty bladder with Foley balloon visible inside. This finding, when coupled with low urine output, narrows the differential diagnosis of oliguria/anuria to (1) ureteral obstruction, (2) intrinsic kidney, or (3) pre-renal disease (see Figure 17). Please click here to view a larger version of this figure.
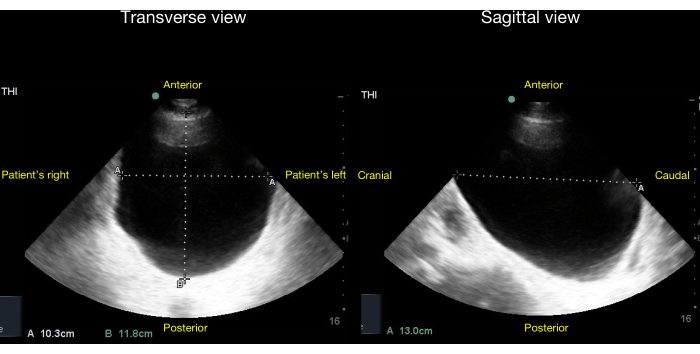
Figure 20: Transverse (left panel) and sagittal views (right panel) of a bladder with no Foley balloon inside and gross bladder distension visible. The volume of urine in the bladder can be quantified by the method described in the Discussion section of this article. After choosing a correction factor of 0.81 for an ellipsoid bladder, the estimated bladder volume in this case = 0.81 x diameter1 x diameter2 x diameter3 = 0.81 * 10cm * 12cm * 13cm = 1,263mL +/- 13%. Please click here to view a larger version of this figure.
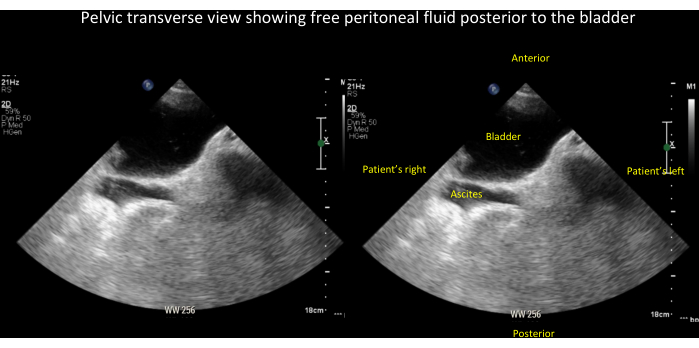
Figure 21: Unlabeled (left panel) and labeled (right panel) images of free peritoneal fluid (in this case, ascites). These are seen posterior to the bladder in the pelvic transverse view (see also Video 15). Please click here to view a larger version of this figure.
Video 1: Fanning through the right kidney in the long view. Please click here to download this Video.
Video 2: Fanning through the right kidney in the short view. Please click here to download this Video.
Video 3: Renal vasculature coming off the aorta. Please click here to download this Video.
Video 4: Renal vasculature with color Doppler. Please click here to download this Video.
Video 5: Kidney in long view with chronic medical renal disease. Note the small size of the kidney. Please click here to download this Video.
Video 6: The right kidney in the coronal plane showing mild hydronephrosis. Please click here to download this Video.
Video 7: The right kidney in the coronal plane showing moderate hydronephrosis, defined by dilation of major and minor calyces, but without cortical thinning. Please click here to download this Video.
Video 8: The right kidney in the coronal plane showing severe hydronephrosis, defined by dilation of major and minor calyces and cortical thinning. Please click here to download this Video.
Video 9: The right kidney in a patient with bilateral extra-renal pelvis. Please click here to download this Video.
Video 10: The right kidney in the longitudinal view with a simple cyst in the center. Please click here to download this Video.
Video 11: The right kidney in the longitudinal view with a larger, simple appearing cyst in the inferior pole of the kidney. Please click here to download this Video.
Video 12: The right kidney in the longitudinal view with a mass in the center. Note that it is not as hypoechoic as the cysts that were previously shown (Video 11). Please click here to download this Video.
Video 13: The right kidney in the coronal plane showing a kidney mass that is arising from the kidney cortex and has disrupted the expected normal oval shape typically seen in this view. Please click here to download this Video.
Video 14: The bladder in a transverse view showing a large, irregular echo density within the bladder lumen that turned out to be a combination of tumor and blood clots. Please click here to download this Video.
Video 15: Pelvic transverse view showing free peritoneal fluid (in this case ascites) posterior to the bladder. See also Figure 21 for a labeled still image of this video. Please click here to download this Video.
