Between 1st September 2022 and 5th June 2023, 25 babies were transported in Western Australia with possible HIE and were eligible for inclusion. Of the total, 20 infants were consented, recruited, and successfully had aEEG applied during their transport. A total of 5 patients were not recruited and 3 were missed for consent. In one case, the device had started an automatic software update and was unusable; in one case, the baby was not at risk of HIE and was deemed ineligible for recruitment. Of the 20 infants, 12 (12/20; 60%) were male and 8 (8/20; 40%) were female. A total of 13 infants (13/20; 35%) were primarily transported by fixed-wing aircraft and 7 (7/20; 65%) by road. In total, 38 h of aEEG traces were recorded. The median postnatal age at which the recording commenced was 5.7 h (3.9-6.5 h) h. Infants primarily transported by fixed-wing aircraft compared to the road had aEEG commenced at 8.9 h (6.2-10.8 h) vs. 4.2 h (3.0-5.5 h); p = 0.0048. The median duration of EEG data recorded per patient was 1.9 h (1.6-3.1 h), with a range of 0.9-6.4 h. There were no impedance notifications in 16/20 recordings. Four recordings had a mean (range) of 4 (1-6) impedance notifications per recording. Despite this, all recordings had information that could be analyzed; examples are shown in Figure 9. The technology was acceptable to parents and staff.
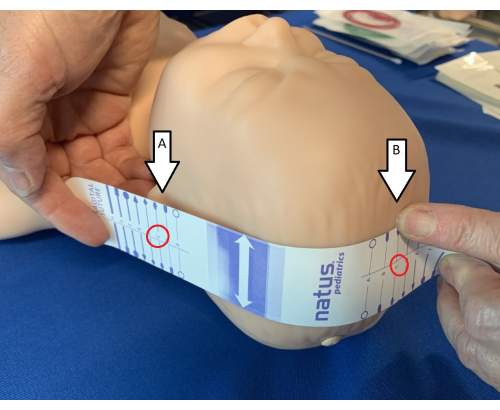
Figure 1: Identification of landmarks for measuring tape. Using the electrode measuring tape, identify the ear tragus (A) and sagittal suture (B) and ensure the tape is lined up so that the letters match (in the mannequin shown in the figure, it is "C"). Please click here to view a larger version of this figure.
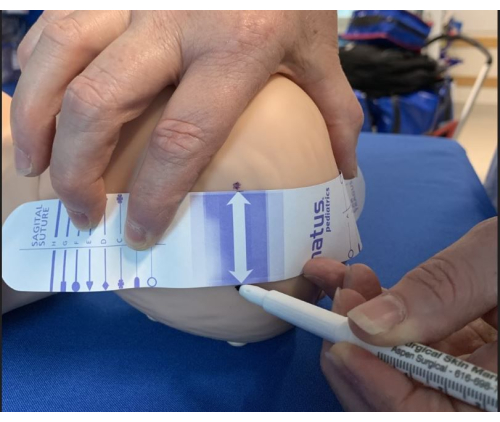
Figure 2: Identifying sites for electrode placement. Once the measuring tape is appropriately positioned to landmarks, mark electrode sites on both sides of the arrow using a marker pen. Please click here to view a larger version of this figure.
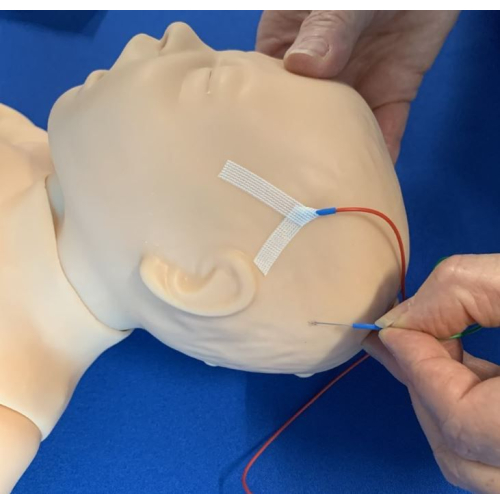
Figure 3: Insertion of electrodes. The electrodes were inserted subcutaneously and positioned caudally, taping with the steristrips Chevron technique. Please click here to view a larger version of this figure.
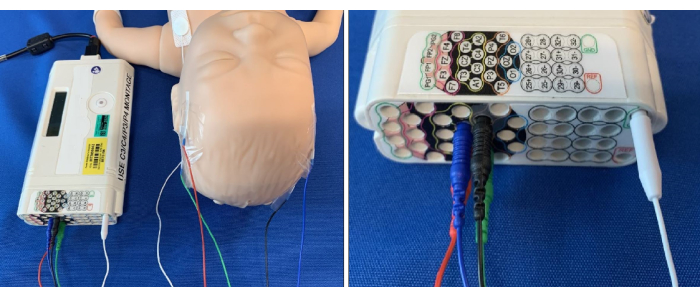
Figure 4: Electrodes connected to the corresponding site on the aEEG amplifier. Please click here to view a larger version of this figure.
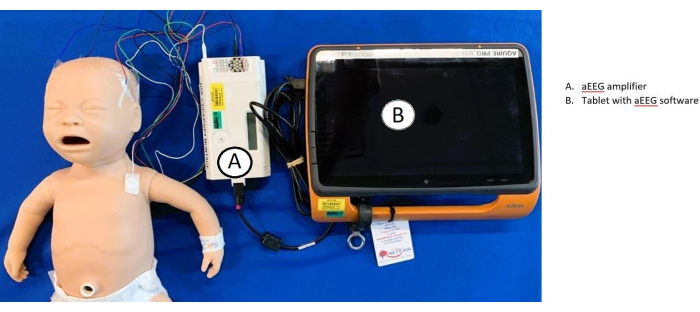
Figure 5: Overview of aEEG set-up and connectivity. Electrodes are connected to the baby and (A) amplifier. The amplifier is then connected to the (B) tablet, which uses aEEG software. Please click here to view a larger version of this figure.
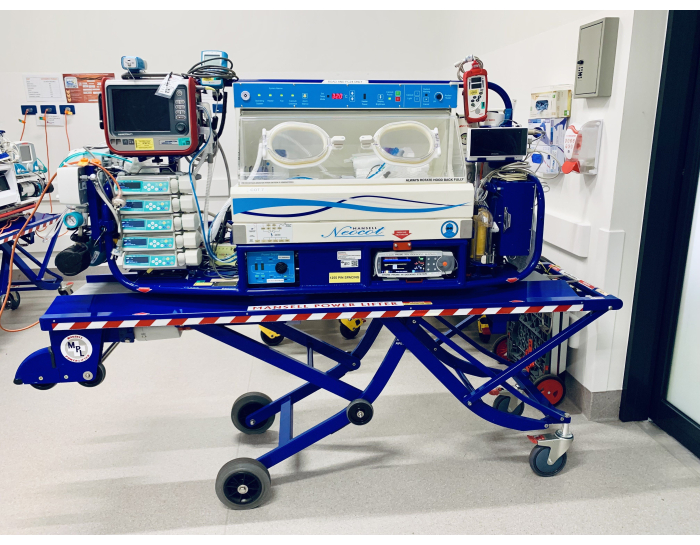
Figure 6: Mansell cot. Please click here to view a larger version of this figure.

Figure 7: Voyager cot. Please click here to view a larger version of this figure.
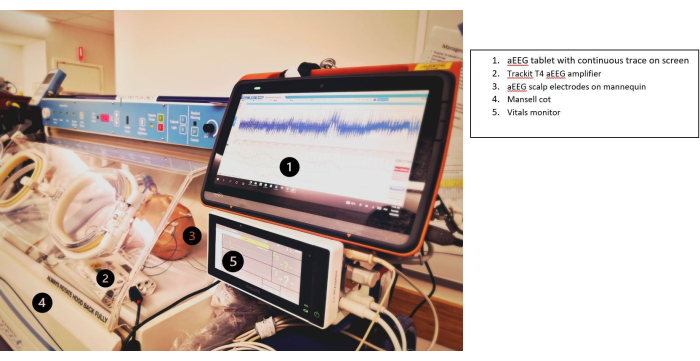
Figure 8: Tablet secured to the cot and visible to the transport team. (1) aEEG tablet with continuous trace on the screen, (2) Trackit T4 aEEG amplifier, (3) aEEG scalp electrodes on the mannequin, (4) Mansell cot, and (5) vitals monitor. Please click here to view a larger version of this figure.
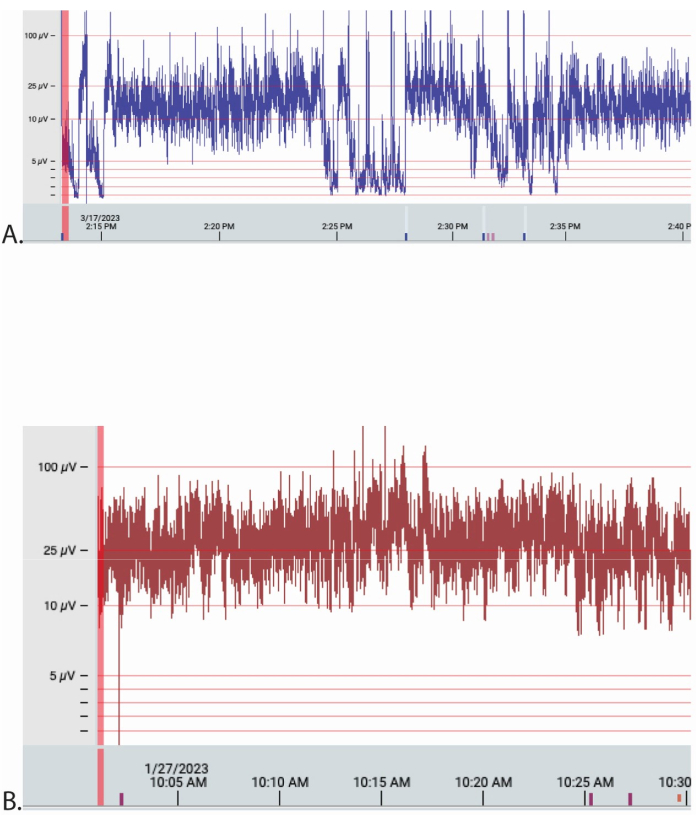
Figure 9: Examples of aEEG traces from 2 patients extracted from the online Stratus EEG Analysis software. The Y-axis is electrical amplitude (µV), and the X-axis is date and time in 5 min increments. The time base was 30 mm/s for each, and the sensitivity was 70 µV/cm for both traces. The traces are montages of the C4-C4, P3-P4 as interpreted by 'experts'. (A,B) Patient A was transported by road and patient B by air. Please click here to view a larger version of this figure.
