Figure 6 shows representative images of pathological changes in HE-stained lung (Figure 6A,B), trachea (Figure 6C,D), and spleen (Figure 6E,F). H1N1 virus infection resulted in inflammatory changes in mouse lungs, including edema and many lymphocytes and neutrophil infiltration. H1N1 virus infection also induced inflammatory changes in mouse tracheae, including cilia shedding and inflammatory cell infiltrations (many lymphocytes and small numbers of neutrophils). In addition, the infection also significantly increased the ratio of the white pulp area to the whole spleen area of mice. Lymphocytes accumulate in the white pulp of the spleen. This standardized procedure for harvesting tissue samples can better evaluate airway inflammation.
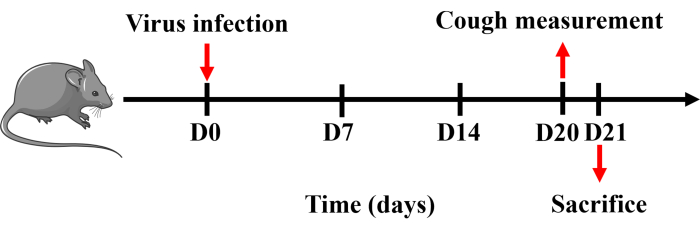
Figure 1: Protocol for establishing a mouse model of cough. Mice were anesthetized with pentobarbital sodium and intranasally instilled with 0.8 x LD50 of H1N1 virus dissolved in 50 µL of PBS once on day 0. Cough measurement was performed on day 20, and mice were sacrificed the following day. Please click here to view a larger version of this figure.
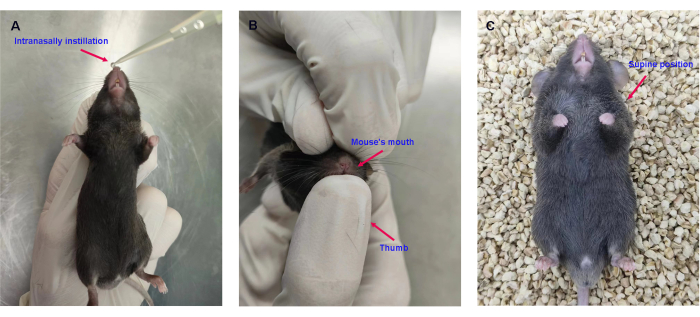
Figure 2: Intranasal instillation of the H1N1 virus. (A) Intranasal instillation of 0.8 x LD50 of H1N1 virus in 50 µL of PBS. (B) Holding the mouse's mouth closed with the thumb. (C) Placing the mice in the supine position. Please click here to view a larger version of this figure.
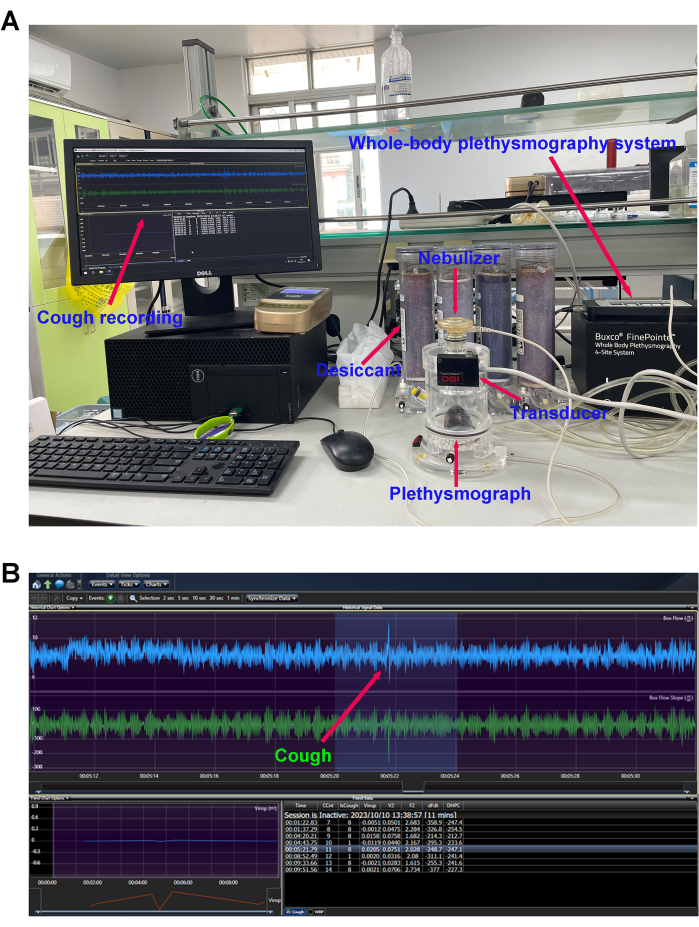
Figure 3: Cough sensitivity measurement. (A) Mouse cough detection equipment and (B) cough reflex curve. The number of cough events in response to the nebulized citric acid solution (0.4 M) was detected using the whole-body plethysmography (WBP) system after modeling. Please click here to view a larger version of this figure.
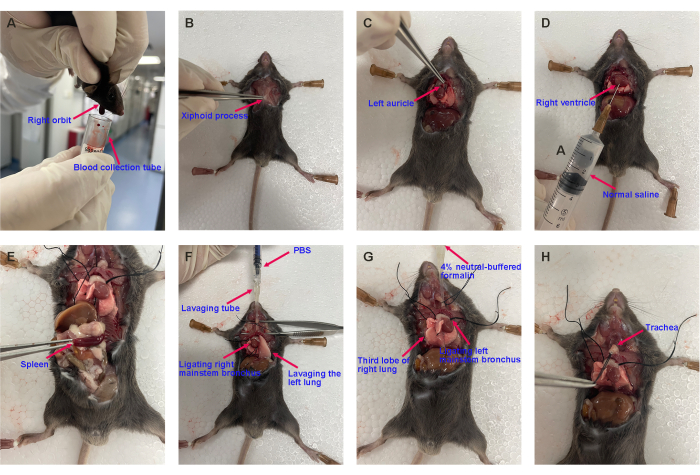
Figure 4: Representative images of harvesting the mouse's blood, spleen, BALF, lung, and trachea. (A) Blood collection, (B) opening the chest, (C) cutting off the left auricle, (D) pulmonary circulation perfusion, (E) harvesting the spleen, (F) bronchoalveolar lavage, and (G) harvesting the lung lobe and (H) the trachea for histopathological analysis. Please click here to view a larger version of this figure.
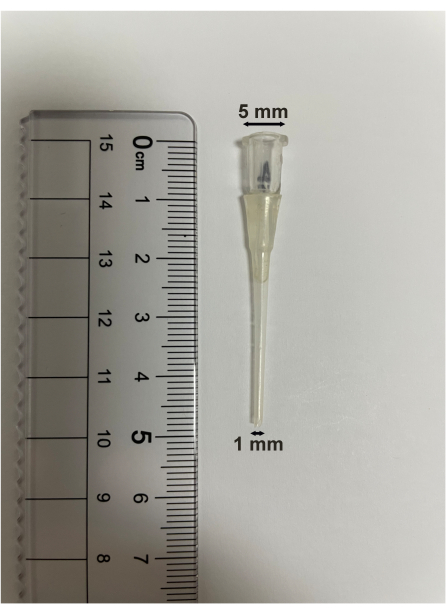
Figure 5: Bronchoalveolar lavage tube specification. The length of the bronchoalveolar lavage tube is 5 cm. The upper diameter is 5 mm, and the lower diameter is 1 mm. Please click here to view a larger version of this figure.
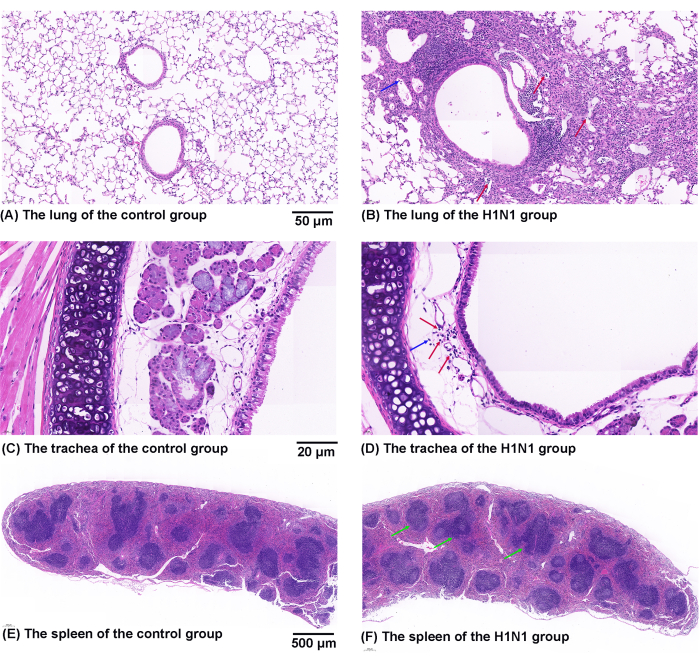
Figure 6: Effects of H1N1 virus on pathological changes in the mouse's lung, trachea, and spleen. (A,B) Representative figures of pathological changes in HE-stained lung sections from the (A) control and (B) H1N1 groups. The symbol of "↑" marks the infiltration of lymphocytes (red) and neutrophils (blue). Scale bars: 50 µm. (C,D) Representative figures of pathological changes in HE-stained trachea sections from the (C) control and (D) H1N1 groups. The symbol of "↑" marks the infiltration of lymphocytes (red) and neutrophils (blue). Scale bars: 20 µm. (E,F) Representative figures of pathological changes in HE-stained spleen sections from the (E) control and (F) H1N1 groups. The symbol of "↑" marks the white pulp (green). Scale bars: 500 µm. Please click here to view a larger version of this figure.
