A schematic overview of the protocol is presented in Figure 1.

Figure 1. Study protocol. The porcine study design of liver injury is based on a donation after cardiac death (DCD) model. After dissection of all liver vessels, cardiac death is induced followed by 45 min of warm graft ischemia. To simulate a graft transport in between the donor and recipient hospitals in a clinical setting, the graft is stored on ice for 4 hr after cold, dual flush. After cold storage, the organ is subnormothermic perfused for 6 hr in order to assess the perfusion stability. In a transplant model, the perfusion time could be shorter in order to recharge energy storage and to assess the organ viability. Please click here to view a larger version of this figure.
1. Animals
NOTE: Male Yorkshire pigs, 30-35 kg, were utilized for this study. All animals received humane care in compliance with the ‘‘Principles of Laboratory Animal Care’’ formulated by the National Society for Medical Research and the ‘‘Guide for the Care of Laboratory Animals’’ published by the National Institutes of Health. The Animal Care Committee of the Toronto General Research Institute approved all studies.
2. Organ Retrieval
- House male Yorkshire pigs in research facilities for 1 week before perfusion/transplantation to reduce the level of stress and to accustom the animals to the housing conditions. Less than 2 days of housing inside the facility will lead to a stress-induced physical reaction, which can alter the perfusion’s outcome22,23.
- Anesthetize pigs by an intramuscular (i.m.) injection of a mixture of ketamine (25 mg/kg), atropine (0.04 mg/kg), and midazolam (0.15 mg/kg).
- Prior to intubation, ensure the pig breathes spontaneously 2 L of O2 dosed with 5% isoflurane. Spray the vocal chords with 2% lidocaine 2 min before intubation to avoid vocal cord spasms. For example, for a 35 kg pig use a 6.5 fr. tracheal tube. Block the tracheal tube with 3-5 ml of room air.
- After intubation, use capnometry to confirm correct intubation. Lower the isoflurane gas to 2%. Set the ventilator to 14-16 breaths/min and a tidal volume of 10 ml/kg bodyweight.
- Place a 20 G intravenous (i.v.) catheter in one of the ear veins to allow infusion of Ringer’s lactate solution (200 ml per hr). Then scrub the pig and cover it with sterile drapes.
- Make a midline incision followed by a left lateral extension. Use a towel to cover large and small bowels and move them to the left side.
- Separate inferior vena cava (IVC) and distal aorta from each other; ligate aorta branches to the back; isolate and free renal arteries from adherent tissue.
- Divide the falciforme ligament and the triangular ligament using cautery.
- Release the portal vein by an incision of the peritoneum between pancreas and portal vein. Tie off veins draining from the pancreas to the portal vein.
- Dissect the coeliac trunk below the portal vein and follow it backwards to the aorta. Surround the mesenteric artery with a 2-0 tie; surround the splenic and left gastric arteries, which branch posteriorly to the coeliac trunk. Dissect the coeliac trunk off the portal vein.
- Ligate the lymph vessels within the hepatoduodenal ligament to prevent lymphatic leakage. Divide the right gastric artery between ties. Ligate smaller veins. Separate the bile duct from the ligament and divide it distally after ligation.
- Dissect the aorta behind the diaphragm between heart and coeliac trunk; place a 2-0 tie around the aorta.
- Release the liver from the lower cava on the right side using electro cautery; use scissors for the upper part between cava and liver.
- Remove the gallbladder and cauterize bleeders from gallbladder bed.
- Administer i.v. 1,000 iU/kg donor weight of Heparin. For a DCD model, induce cardiac arrest by intracardial injection of 40 mval KCl 3 min after Heparin administration. Set cardiac arrest as the starting point of warm ischemia.
- For the perfusion, collect 1.6 L of pig blood in CPDA bags (citrate, phosphate, dextrose, adenosine) immediately after cardiac death. Perform a soft spin (2,000 x g without brake). Remove the plasma and the buffy coat under sterile condition (biosafety cabinet class II) and store the erythrocytes in CPDA bags for transfusion.
- Cannulate portal vein and aorta with organ flush lines. Tie off the previously set ties around femoral, renal, splenic, mesenteric, and left gastric arteries as well as the upper aorta. For a heart beating donor (HBD) model, perform the cannulation of aorta and portal vein under heart beating conditions.
- After 45 min warm ischemia, flush the liver with University of Wisconsin (UW) solution using dual perfusion via aorta (pressure bag) and portal vein (gravity driven).
- Cut the liver out of the pig, leaving all remaining vessels long.
- During back-table preparation, clamp the upper IVC using a Satinsky clamp and flush the liver a second time with about 0.5 L of UW solution retrogradely via lower IVC until the portal vein outflow is clear.
- Tie off all arterial branches from the aorta and coeliac trunk. Perform an arterial back-table pressure perfusion with about 0.5 L of UW solution.
- Flush the bile duct using UW solution.
- Cannulate the upper and lower parts of the IVC using 1/2” x 3/8” reducers with Luer Lock; cannulate the portal vein and liver artery using 3/8” x 1/4” and 1/4” x 3/8” reducers with Luer Lock. Use the upper and lower vena cava as venous drainage.
- Place the liver in an organ bag, close the organ bag, and store the liver on ice until the perfusion has started.
3. Ex vivo Liver Perfusion
- Prepare the perfusion solution containing 2,000 ml Steen solution, 400 ml washed erythrocytes, 550 mg sodium pyruvate, 100 ml amino acid solution (10% Travasol), 10 mg calcium gluconate, 1,000 IE rapid acting insulin, 1 g cefazolin, 500 mg metronidazol, and 10,000 iU heparin. Add other molecules for vasodilatation, immunosuppression, scavenging of reactive oxygen species, or liver cell treatment based on the particular study protocol.
- For the dialysis component, use standard dialysate containing 3.5 mM potassium, 25 mM bicarbonate, 27 mM glucose, as well as 275 mg/L pyruvate.
- Set up the perfusion circuit (schema see Figure 2).
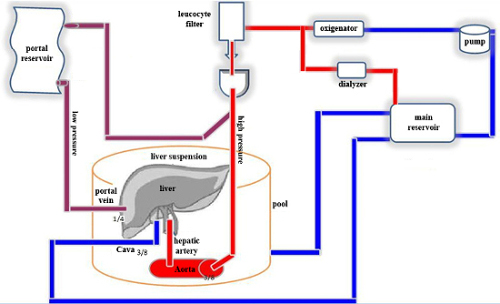
Figure 2. Circuit set up. Coming from the main reservoir as the starting and end point, the perfusion solution is driven by a centrifugal pump through an oxygenator. Right after oxygenation of the solution, the circuit splits into a smaller line running to a dialyzer unit for electrolyte homeostasis and a bigger line running to a leukocyte filter for reduction of remnant white blood cells (WBC). The solution that runs through the dialyzer returns to the main reservoir. After the leukocyte filter, the circuit splits up again into 2 equal lines. One line runs at high pressure (around 60 mmHg) directly into the aorta to perfuse the hepatic artery. The other line drains into a second reservoir. From this reservoir the portal vein is perfused. The pressure of the portal perfusion depends on the elevation energy of the reservoir’s solution level (around 2-6 mmHg). All fluids are drained via the infra- and supra-hepatic cava back into the main reservoir. For gravity reduction and homogeneous perfusion, the liver is placed in a pool filled with temperature regulated water. It is separated from the water by an impermeable membrane and it swims in a perfusion suspension. Please click here to view a larger version of this figure.- Collect all fluids from the circuit in a 3 L reservoir (main reservoir) and clamp the outflow.
- Connect the outflow to a centrifugal pump followed by a commercial oxygenator.
- Behind the oxygenator, split up the tubing into 2 lines. Connect one line to a dialyzer and drain it back into the main reservoir. Connect the second line to a leukocyte reduction filter.
- Split up the line after the leukocyte reduction filter into an arterial line, which supplies perfusion solution to the hepatic artery, and a portal venous line delivering perfusion solution to a second reservoir, which drains into the portal vein by gravity outflow. Clamp the portal inflow.
- Connect the arterial line to a vena cava line draining into the main reservoir for fluid recollection.
- For collection of ascites or leakage of perfusion solution from the liver, prepare a suction line connected to the main reservoir.
- Release the outflow clamp from the main reservoir and fill the circuit with the perfusion solution. Start the centrifugal pump at 1,500 rounds/min. The perfusion solution will drive through the arterial line into the vena cava line back into the main reservoir. Make sure all air is driven out the circuit.
- Turn on the gas supply to the oxygenator.
- Take the liver off the ice. Flush out the UW solution using saline.
- Place the liver, with its convex side down to facilitate the access to the vessels, ideally in a gravity-free environment to avoid organ compression at the contact surface. Use a heat- and coolable water bath. Set the starting temperature of the circuit and water bath to 20 °C. Cover the water bath with an impermeable membrane and place the liver onto that membrane. Reduce gravity driven compression by submerging the liver with perfusion solution.
- Reduce the speed of the centrifugal pump to 1,000 rounds/min and place two clamps at the connection of arterial and vena cava lines. Then, cut the tubing in between the clamps. Using a 3-way connector, join both cava outflows and connect them to the vena cava line.
- Release the clamp from the arterial line, pour perfusion solution into the arterial cannula to get rid of bubbles, and connect the line to the cannula. Increase the centrifugal pump to 1,500 rounds/min. Release the second clamp from the vena cava line.
- Release the clamp from the portal venous reservoir in order to fill it up. Let perfusion solution pour into the portal cannula and connect it. Take special care of stable fluid levels in the portal reservoir.
- Connect pressure lines to the Luer Locks of the arterial, portal, and vena cava cannulas.
- To mimic physiological conditions, apply treatments into the right vessel. Inject glucose into the portal vein and not into the arterial line in order to establish a gradient mimicking an increased portal venous glucose gradient and inducing glycogen synthesis24,25.
- After connecting the liver to the circuit, raise the temperature to 33 °C within 60 min.
- Aim for an arterial starting flow at about 250 ml/min at 40 mmHg. This may reach 700 ml/min during perfusion once the pressure is increased up to 70 mmHg.
- At starting temperature, aim for a portal vein flow of 500-600 ml/min at 3-5 mmHg. After raising the temperature, monitor the portal venous flow, which will increase up to 1,100 ml/min at 4-6 mmHg. Avoid exceeding portal pressure above physiological values (around 8 mmHg) to protect sinusoidal fenestrations26. Avoid exceeding total flow above 2,000 ml/min in order to prevent damaging the organ. Set the outflow to -2 mmHg by lowering the main reservoir to prevent liver congestion by functional outflow obstruction.
- Add the dialysis component to the circuit in order to equilibrate the perfusion solution to predetermined values27. Set the dialysate flow to 500 ml/hr. Take special attention to adjust the dialysis outflow so that the perfusion solution is neither diluted nor concentrated. Within the first hour of perfusion the main reservoir must be watched carefully!
- Ensure homogeneous oxygenation of the tissue to recover and maintain organ function by using a main gas mixture component of O2 (95-98%) and CO2 (2-5%). Use variable gas during perfusion since the liver changes its metabolism and its pH demand during perfusion.
- Maintain a low pH during the start of perfusion to protect the organ using the paradox pH concept28 and avoid severe tissue damage that can result from fast connections to physiological pH under reoxygenation, since after storage in UW solution, the organ has an acidotic pH below 7. Adjust the partial pressure of CO2 continuously down to 25-30 mmHg so that the pH will reach a physiologic level within 1 hr.
- Add sodium- or potassium bicarbonate to the circuit to achieve a physiological concentration of standard bicarbonate in the perfusion solution. Inject it carefully under repetitive blood gas and electrolyte control.
- Monitor the perfusion by periodical venous and arterial blood gas and AST analyses. The venous PO2 remains above 175 mmHg during the perfusion. Monitor vascular flow and pressure and note a stable perfusion by a constant vascular resistance.
- Keep the perfusion system stable for up to 8 hr. At the end of the ex vivo perfusion period, cool down the perfusion system to 20 °C and, after disconnecting the circuit’s tubing from the liver, flush the perfusion solution out the liver dually with ice cold UW solution. Store the liver once again placed on ice in a sterile organ bag.
Below, we present the results of 5 perfusion experiments with DCD-grafts after 45 min warm- and 4 hr cold ischemia prior to the start of the subnormothermic ex vivo perfusion.
The main goal for an ex vivo liver perfusion is to ensure a sufficient oxygen supply to the organ. Ischemia causes vasoconstriction, thus increasing the perfusion resistance. Achieving constant vascular flows with stable pressures is a good indicator of adequate oxygenation. During an induction period of 1-2 hr the perfusion solution and the organ are warmed up to 33 °C, which deceases the vascular resistance of the liver. Once the target temperature of 33 °C is achieved, flow values level at a constant, nearly physiological range for the rest of the 6 hr perfusion time (Figures 3A-3D).
At the same time, the organ becomes metabolically active. Figure 4A shows the venous pO2, a marker of oxygen consumption. Within the initial 2 hr the venous pO2 declines to a constant plateau. At this metabolically active state, the liver starts producing bile (Figure 4B). The dialyzer provides a balanced electrolyte homeostasis (Figures 4C-4D). An initial hyperkalemia is quickly leveled out. Online AST measurement serves as monitoring of hepatocellular damage. Figure 5 displays only a shallow linear AST increase over the entire perfusion period. H&E staining after 6 hr of perfusion reveals hepatocyte necrosis <5 % with an intact lobular and sinusoidal structure (Figure 6). PAS staining at the same time point shows replenished cellular glycogen storage compared to exhausted storage in cold preserved DCD-grafts (Figure 7).
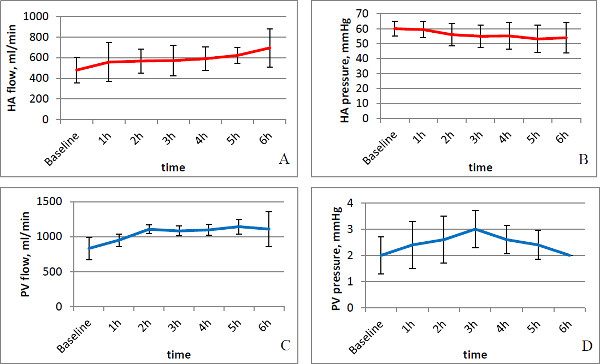
Figure 3. Perfusion flows and pressure (n = 5, error bars show standard deviation). (A,B) Hepatic artery (HA) flow and pressure: During the warming phase in the first 1-2 hr, the flow increases at stable pressures and is constant afterwards. Looking at the decreasing portal venous pressure (C), the increase of HA flow towards the end of the perfusion might be an autoregulatory reaction of the liver. (C,D) The portal venous (PV) flow increases corresponding to the HA flow during the first 2 hr of warming. The pressures remain relatively stable.
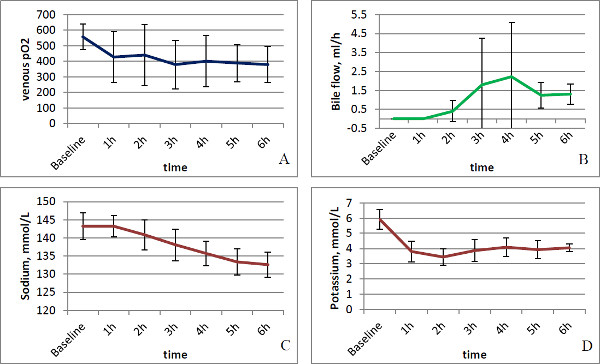
Figure 4. Monitoring parameters (n = 5, error bars show standard deviation). (A) The venous pO2 as a marker of oxygen demand and metabolic activity decreases within the initial phase of warming due to activated cellular metabolism; it remains stable afterwards. (B) Bile production as a marker of metabolic activity starts at temperatures around 30 °C and, thus, between the first and second hour of perfusion. (C,D) The dialyzer assures electrolyte homeostasis; an initial hyperkalemia is quickly balanced.
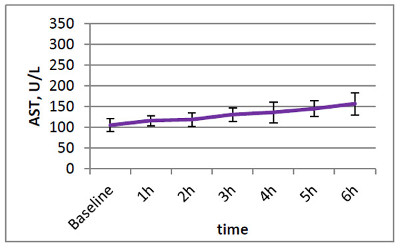
Figure 5. AST (n = 5, error bars show standard deviation). AST is a sensitive marker of hepatocellular injury; the shallow increase suggests no significant injury during ex vivo perfusion.
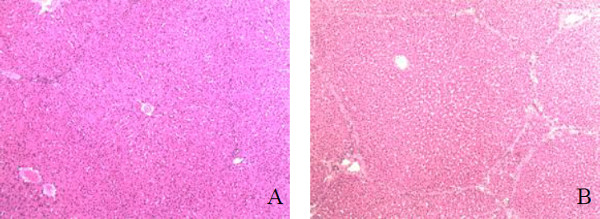
Figure 6. H&E staining (20X magnification). (A) Sham liver sample before warm ischemia, one representative liver lobule with intact architecture. (B) Liver sample after 45 min of warm ischemia, 4 hr of cold ischemia, and 6 hr of subnormothermic perfusion, the lobular architecture is intact without necrosis and only minimal cell swelling, the sinusoidal spaces are mildly dilated in comparison to the sham sample.
