Using this enzymatic digestion protocol, we have consistently been able to isolate and grow MF population gut CD90+ mucosal stromal cells from GI surgical specimens and biopsies (Figure 1). Visible MF colony proliferation could be observed on day 2 – 5 after seeding mononuclear cell suspensions into 6 well plates (Figure 1A-B). The MF primary cultures reach ~ 50 – 70 % confluence by day 7 – 11 (Figure 1C-D).
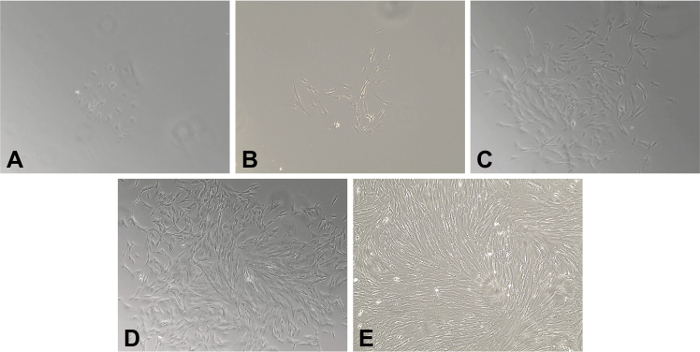
Figure 1. Primary Myofibroblasts (MFs) Isolated from Frozen Gastrointestinal Tissue. A 20X magnification of human MFs isolated from frozen specimen of human colonic mucosa. (A) Day 2. Adherent clusters of stromal cells are present. (B) Days 4. The characteristic spindle- or stellate-cell morphology has developed and is readily apparent. The density of fibroblast continue to increase on (C) Day 7 and (D) Day 10. (E) By Day 14, there is a completely confluent monolayer of MFs. Please click here to view a larger version of this figure.
There is a slight decrease in viability of mucosal single cell preparation upon the freezing of surgical specimens (~10%, Table 1). However, with freezing, there is also a decrease in the bacterial/fungal contamination of the tissue observed and consequently, an increase in the efficiency of the MF culture generation.
| Source of GI Mucosal Myofibroblasts | Viability* of Mucosa Single Cell Suspension Preparation (n = 11) | MF Isolation Efficiency (n = 11) |
| Fresh | 88.32 ± 2.369 | 8 out of 11 (82%) |
| Frozen | 78.64 ± 4.174 | 11 out of 11 (100%) |
| *Viability as determined by automated cell counter following 0.4% trypan blue solution staining. | ||
Table 1. Viability and Efficiency of Myofibroblast Recovery. Fresh vs. Frozen Tissues.
The purity of generated MF culture was analyzed after cells were propagated at least for two passages, in order to ensure no contamination by other mucosal cells. Using confocal microscopy, it was demonstrated that MFs were positive for the marker of the mesenchymal cell lineage CD90 and vimentin, and also α-SMA, a marker of the differentiated mesenchymal cells (Figure 2).
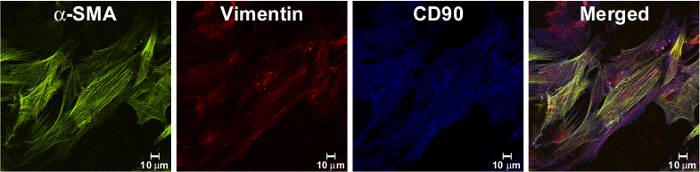
Figure 2. Isolated Cells Have Fibroblast Shape and Express MF Markers. Immunostaining of isolated MF monolayer, passaged at least two times in culture were fixed with 1% paraformaldehyde, immunostained and analyzed by confocal microscopy as described previously9. Isolated cells expressed a marker of myofibroblast, a-SMA (in green, as detected by murine mAb clone 1A4), and mesenchymal markers: vimentin (in red, as detected by mAb, clone RV202) and CD90 (in blue, as detected by murine mAb, clone 5E10). In the merged image, orange/yellow cells represent co-localization of a-SMA and vimentin; purple represents co-localization of vimentin and CD90. Please click here to view a larger version of this figure.
This data was confirmed by flow cytometry analysis (Figure 3). As previously reported, normal MFs isolated from GI mucosa also were negative for hematopoietic makers CD45 and CD31, as well as epithelial marker, EpCAM3, 5, 9.
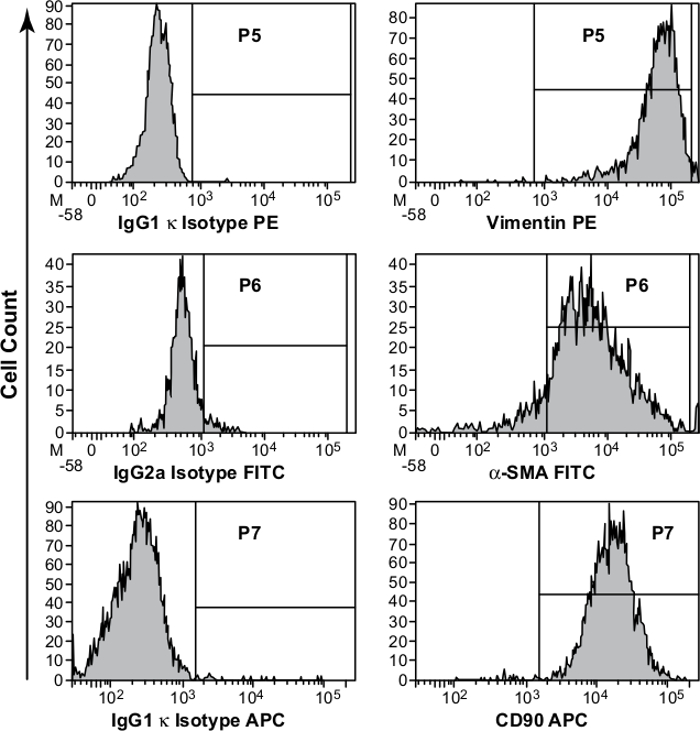
Figure 3. Phenotypic Characterization of Primary Myofibroblast (MF) Cultures. Studies were performed on primary MFs isolated from colonic mucosa and passaged at least two time in culture. Immunostaining, followed by flow cytometry analysis, confirmed that the isolated cells have MF phenotype are uniformly positive for vimentin, α-SMA, and CD90. Appropriate isotype controls were included in the study. Please click here to view a larger version of this figure.
