The study was approved by the Research Ethics Board of the University Health Network. Signed informed consent was obtained from each participant before enrollment in the study. Signed informed consent was also obtained from any caregivers or household members appearing in video recordings.
1. Verification of the protocol applicability to the individual
NOTE: This protocol is intended to be applied to individuals with impaired but not completely absent hand function (specific criteria can be adapted to the population and/or question of interest).
- Ask participants whether their affected hands impact their ability to carry out ADLs.
NOTE: It is recommended to ask participants to give some examples of tasks that they can and cannot perform independently with their affected hands. - Verify that the total score on the Montreal Cognitive Assessment (MoCA) is above 21, in order to avoid potential difficulties understanding and following protocol procedures.
2. Determination of the daily routine of participants
- Ask participants to recall their daily routines over the past two weeks. Document which daily tasks are performed, for how long, and at approximately what time.
- In collaboration with participants, select 3 timeslots of 1.5 h each during which to record videos. Select timeslots that are spread over different days of the week, and take place when ADLs involving the hands are typically carried out in sequence.
NOTE: The selected ADLs must be representative of each participant's typical activities, and be perceived by them as meaningful. Scheduling recording periods on different days is intended to increase the variety of recorded ADLs and to promote the capture of useful and meaningful data.
NOTE: Recording timeslots are scheduled for recording efficiency, but participants should understand that they have full control of when to start and to stop recordings.
3. Agreement on recording schedules and target video content with participants
- Obtain agreement of each participant on the recording schedules, after discussing any concerns that they may have.
- Set a goal of 3 h of videos over two weeks. Inform participants that insufficient videos may lead to extending their recording periods.
4. Emphasis of the importance of performing ADLs naturally
- Instruct participants to focus on capturing realistic routines, instead of specifying particular activities to record. The intent of the instruction is to discourage participants from artificially recording specific activities in greater amounts than is typical for them.
5. Notification of potential privacy issues during recordings at home
- Ensure that participants understand that all recordings should take place inside their homes, not in public places to avoid privacy issues.
- Give some examples that may raise privacy concerns, such as bathing, dressing/undressing, and checking confidential information. Remind participants to be aware of mirrors, which may show their faces in the recordings.
- Suggest that participants avoid the presence of other people such as family members or caregivers as much as possible in the videos.
NOTE: In the context of research studies, in cases where the presence of other people is unavoidable, informed consent should be obtained from those individuals.
6. Camera and tablet instruction
NOTE: If participants indicate during the initial contact that they require caregiver assistance for many of their daily needs, the caregiver is encouraged to also attend the study visit and be trained on the use of the equipment, so that they can later assist the participant.
- Demonstrate how to use an egocentric camera (Table of Materials) to participants.
- Demonstrate how to turn the camera on and off.
- Demonstrate how to control recordings (start, pause, stop) using the camera.
- Demonstrate how to use a tablet (Table of Materials) with the preinstalled camera app to control the recordings, if applicable.
NOTE: The demonstration includes controlling the recordings from the camera app, as well as replaying and editing (e.g., trim or delete) the recorded videos. A camera remote was initially considered (Supplemental Files), but in practice was not used because participants were comfortable using the camera or tablet to start and stop recordings.- Demonstrate how to turn on and off the tablet.
- Demonstrate how to connect the tablet to the camera through the camera app.
- Demonstrate how to control the recordings from the camera app.
- Demonstrate how to review recorded videos from the camera app.
- Demonstrate how to trim or delete the videos from the camera app.
- Demonstrate how to don and doff the camera using an elastic headband adjustable to the participant's head.
NOTE: See Figure 1.
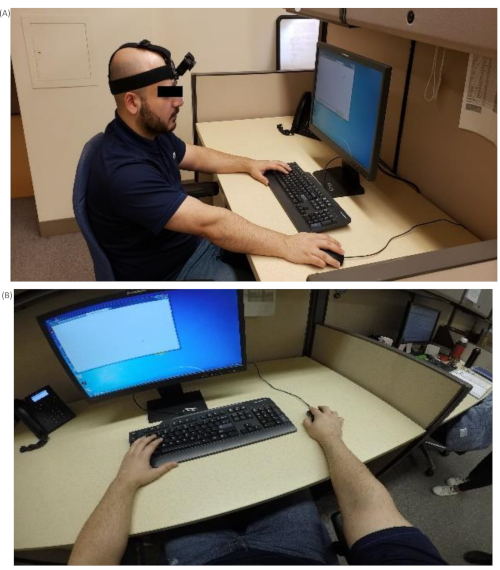
Figure 1. Wearable camera setup. (A) Positioning of the egocentric camera. (B) Viewing angle from the camera. Please click here to view a larger version of this figure.- Place the camera on the participant's forehead. Adjust the headband to wear the camera comfortably and steadily.
- Ensure an optimal angle of the camera with respect to the forehead.
- Ask participants to record a short segment of video while moving the hands in front of them and manipulating an object (e.g., the tablet).
- Review the recorded video and ensure the two hands were clearly visible in the central region of the scene while conducting manipulation tasks.
- Practice the use of the camera and tablet with participants and their caregivers, until they demonstrate proficiency.
7. Giving the equipment
- Give the kit with all the equipment to participants to record their ADLs at home. In addition to the camera and tablet, the kit includes extra camera batteries, battery chargers for both camera and tablet, charging cables, headband for the camera, and a printed set of guidelines for using the camera (See the Supplemental Material).
8. Experimental troubleshooting and followup
- Provide contact information of the researchers to help solve obstacles during the actual recordings at home. After one week, researchers call the participants to document the recording progress and solve any potential technical issues.
9. Retrieval of equipment and videos
- Retreive all the equipment and videos from participants in person or through pre-paid mail parcels.
- Ensure that participants agree to share all the videos returned. Participants are encouraged to review all of the collected videos before returning them to the research team, and to delete any portions that they do not wish to share.
- For research studies, review the returned videos and check if anyone appears in the video without having given their consent. If so, send consent forms or call the individuals who appear in the videos to gain their consents for use of the videos. If the individuals are not reachable, the portions of the videos in which they appear are deleted by the researchers.
Participant demographics and inclusion criteria
A sample of 23 participants was recruited for these studies: 9 stroke survivors (6 men, 3 women) and 14 individuals with cSCI (12 men, 2 women). Summary demographic and clinical information for the recruited sample are reported in Table 1.
| Age (years) | Duration after injury (months) | Etiology | Level of Injury | Upper Limb Function Assessment (Mean ± SD) | |||
| Level of Injury | AIS | UEMS: Right Hand | UEMS: Left Hand | ||||
| cSCI (N=14) | 55.9 ± 7.1 | 56.4 ± 58.9 | 12 Traumatic | C4 – C8 | A – D | 18.1 ± 6.2 | 18.6 ± 6.4 |
| 2 Non-traumatic | |||||||
| Stroke (N=9) | 56.8 ± 19.3 | 94.4 ± 134.4 | 5 Ischemic | FMA-UE: Affected Hand | ARAT: Affected Hand | ||
| 4 Hemorrhagic | 45.6 ± 17.3 | 37.1 ± 19.1 | |||||
| AIS: ASIA Impairment Scale; UEMS: Upper Extremity Motor Score | |||||||
| FMA-UE: Fugl-Meyer Assessment for Upper Extremity; ARAT: Action Research Arm Test | |||||||
Table 1. Demographic and clinical information of the recruited participants.
The mutual inclusion criteria for both groups in these studies were: 1) over 18 years old, 2) impaired but not absent hand function, 3) absence of other neuromusculoskeletal disease affecting upper limb movements, 4) no deformity of upper limbs joints, and 5) absence of pain when moving upper limbs. Additional inclusion criteria for each of the two groups were as follows.
For individuals with cSCI: 1) neurological level of injury between C4 and C8 according the International Standards for the Neurological Classification of Spinal Cord Injury (ISNCSCI), 2) American Spinal Injury Association Impairment Scale (AIS) grade A-D. 3) Traumatic or non-traumatic injuries, 4) A unilateral ISNCSCI Upper Extremity Motor Score (UEMS) between 10 and 23 for at least one limb.
For individuals with stroke: 1) at least 6 months post-stroke, 2) total score on the Action Research Arm Test (ARAT) greater than 10, 3) Montreal Cognitive Assessment (MoCA) score above 21 to avoid potential difficulties understanding and following study procedures.
Content and length of recorded video
The videos used for the analysis presented here were from 22 of the 23 participants. The remaining participant (man with cSCI) returned the camera without any usable data after being out of touch with the research team for close to 6 months, and is not included in the remainder of the analysis. As such, the proposed protocol was successful for 95.7% of the participants. On average, participants recorded more than 5 activities. Activities included in the video recordings were meal preparation, eating, dishwashing, physical activity, and knitting (Figure 2). An average of 3.11 ± 0.98 h of video were obtained per participant, after discarding segments where other individuals were present who did not provide consent or where the data was not usable at all (e.g., camera was left recording on a table). In addition, the daily average video recording length per participant was 60 ± 33 min. Three participants postponed the recordings due to illness. Most participants recorded video following the agreed schedules, but they reported feeling tired and uncomfortable wearing the camera for over 1 h due to its weight and heat against the forehead. Additional recordings were scheduled to fulfill the 3 h video duration target when necessary. The average recording period required to acquire 3 hours of video was 22.3 ± 12.9 d. The recording periods ranged from 12 to 69 d, counting from the day the participant was given the camera to the day they returned it. In 4 instances, the length of videos obtained was lower than the 3 h target due to health conditions or scheduling constraints. Two participants took more than 2 months to record 2 h of videos due to family responsibilities. Another participant recorded nearly 2 h of videos over two weeks and then decided to return the camera because of travel plans. Another participant accidentally deleted all recorded video, and after being scheduled for additional recordings was able to provide only 1 h of video due to family responsibilities.
In addition to variations in duration, hand visibility influenced the quality of the videos. Some recorded activities did not show the hands clearly, such as physical training and reaching for objects in over-head cabinets. Hands were not shown in 3 ADLs from two participants with stroke. Regarding physical training, one participant was using an elastic band for upper limb exercises and playing tennis in the backyard. Hands in the video were not always visible since the arm movements were large and fast. Apart from the activities requiring upper limb movements with a wide range, most recorded ADLs were carried out within a workspace between the waist and shoulder, with the hands visible in the recordings.

Figure 2. Examples of two frequently recorded ADLs from the videos obtained. (A) Meal preparation. (B) Dish washing. Please click here to view a larger version of this figure.
Assistance required
Six out of twenty-two (27%) participants required assistance from the research team during the recording periods at home. On average, each help call took 5-10 min. No home visits were necessary. The difficulties encountered related to battery changing, Bluetooth connection, Wi-Fi connection, reviewing and trimming videos on the tablet, and controlling the recordings from the tablet. To solve these issues the following strategies were adopted:
As changing batteries may be difficult for individuals with impaired hand function, the researcher suggested to use the charging cable to recharge the camera. For technical issues related to camera-tablet connections (e.g., Wi-Fi and Bluetooth problems) as well as for reviewing videos on the tablet, the researchers verbally guided participants through the procedures step by step. For the issues related to trimming videos, assistance was provided when participants returned videos to the researchers in person to avoid unintentionally deleting other recorded videos. In case participants were not able to use the tablet to start and stop the recordings, they were told to use the camera alone, by clicking the recording button to control the start and stop of the video recordings.
Privacy concerns
Consistent with previous findings21, most participants and their family members did not report privacy concerns about recording ADLs at home. One family member of a participant was unwilling to be included in the video, and the participant was able to avoid the situation. In total, one participant was assisted with trimming the returned videos. Qualitative analyses of participants' views on the collection of egocentric videos at home will be reported elsewhere, however, privacy considerations did not result in any obstacles to the data collection in these studies. In this protocol, the ADLs were recorded in home environments in order to avoid privacy concerns in public spaces. Apart from the participants, 15 bystanders (including caregivers and family members) of participants were included in the returned videos and consented to their inclusions in the study. Among the 15 bystanders included in the videos, 6 of them were not identifiable since their faces were not shown. In addition, approximately 20 min of videos from 2 family members of participants with stroke were discarded because portions of the videos showed their faces without their consents.
Supplemental Material. Please click here to download this file.
