Functional analysis
The representative results of this study arise from 6 animals and the data shown are mean ± standard error of the mean.Renal function is assessed by determining the urine output, estimated glomerular filtration rate (eGFR), plasma creatine, and blood urea nitrogen (BUN). The biomarkers of renal function are assessed using a portable chemistry analyzer. eGFR is calculated according to the following formula: eGFR =1.879 × BW1.092/PCr0.6 (BW: body weight in kg; PCr: plasma creatinine in mg/dL)10,11.
Following 60 min of bilateral renal artery occlusion, urine output was significantly decreased from 3.6 mL/kg/h ± 0.5 mL/kg/h to 0.2 mL/kg/h ± 0.1 mL/kg/h (p < 0.01). This decrease remained significant at 6 h (1.2 mL/kg/h ± 0.1 mL/kg/h; p = 0.02 vs. baseline) and 24 h (1.3 mL/kg/h ± 0.4 mL/kg/h; p = 0.02 vs. baseline) following reperfusion. Similarly, a significant decrease was observed in eGFR, which dropped from 2.5 mL/kg/h ± 0.1 mL/kg/h at baseline to 1.7 mL/kg/h ± 0.1 mL/kg/h (p < 0.001) at the end of ischemia and to 1.5 mL/kg/h ± 0.1 mL/kg/h (p < 0.001), 1.2 mL/kg/h ± 0.1 mL/kg/h (p < 0.001) and 0.9 mL/kg/h ± 0.1 mL/kg/h (p < 0.001) at 2 h, 6 h and 24 h reperfusion, respectively (Figure 2A-B).
Plasma creatinine was significantly increased at 2 h (2.7 mg/dL ± 0.2 mg/dL; p < 0.01), 6 h (3.7 mg/dL ± 0.3 mg/dL; p < 0.001) and 24 h (5.6 mg/dL ± 0.7 mg/dL; p < 0.001) of reperfusion compared to baseline (1.1 mg/dL ± 0.1 mg/dL). BUN was 6.5 mg/dL ± 0.8 mg/dL at baseline and increased to 17.8 mg/dL ± 3.3 mg/dL (p < 0.001) and 36.2 mg/dL ± 2.9 mg/dL (p < 0.001) at 6 h and 24 h of reperfusion, respectively (Figure 2C-D).
Gross anatomy and histology
There were evident necrotic and hemorrhagic areas which were unevenly distributed in both kidneys at the end of the 60 min of bilateral renal ischemia and the 24 h of reperfusion (Figure 3A). Masson's Trichrome staining revealed confluent coagulative necrosis which was located at the proximal tubules of the renal cortex. (Figure 3B). Plastic embedded sections (1 µm) were also assessed since they provide significant details of the histology (Figure 3C). All Masson's Trichrome slides were evaluated for cell necrosis, loss of brush border, cast formation, and tubule dilatation. Then, a semi-quantitative scoring system for acute tubular necrosis (ATN) was implemented as follows: 0 if none; 1 if less than 10%; 2 if between 11%-25%; 3 if between 26%- 45%; 4 if between 46%-75%; and 5 if greater than 76%. ATN scoring showed significant injury in the renal cortex (score of 4.5 ± 0.3) and considerable injury in the medulla (score of 2.7 ± 0.4).
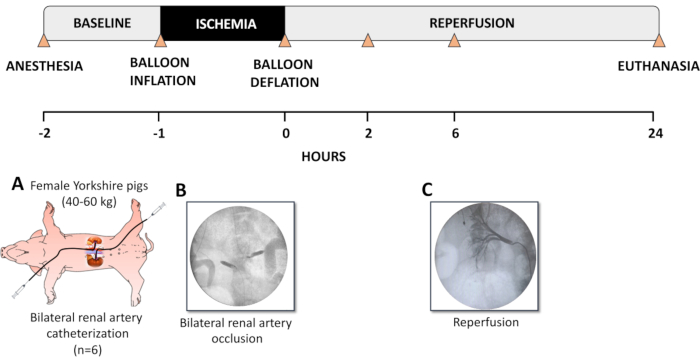
Figure 1. Description of the experimental model. (A) Female Yorkshire pigs (40-60 kg) were sedated and intubated. The left femoral artery and the right carotid artery were catheterized with a 5F angiography sheath. Right jugular venous lines and a Foley urinary catheter were also placed. Selective catheterization of the renal arteries was performed using a 5F multipurpose guide-catheter. (B) Occlusion of the renal arteries was performed using a 5F percutaneous transluminal angioplasty (PTA) dilatation catheter inflated in the proximal portion of the renal artery, totally occluding the blood flow to the kidneys for 60 min. Confirmation of the occlusion was acquired by injection of iodinated contrast medium in the aorta and by checking for any opacification of the vessels of the kidneys. (C) Following 60 min of occlusion, the balloons were deflated and carefully removed. Angiography was performed to confirm renal artery patency and the establishment of renal reperfusion. The animals were then allowed to reperfuse the kidneys under physiological conditions for the next 24 h and were subsequently euthanized. Blood and urine samples were collected right before and after bilateral renal ischemia, at 2, 6, and 24 h after occlusion (timepoints indicated with triangles). This figure has been modified from Doulamis et al11. Please click here to view a larger version of this figure.
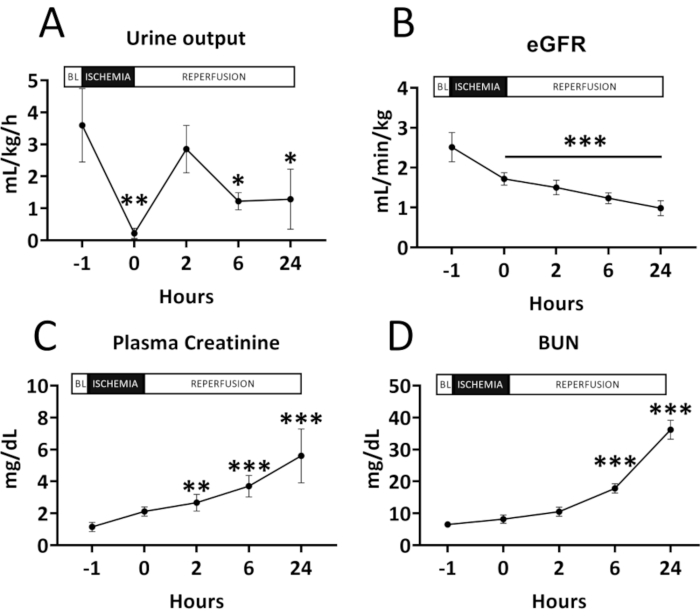
Figure 2. Renal function before and after renal ischemia-reperfusion injury. (A) Urine output; (B) Estimated glomerular filtration rate (eGFR); (C) Plasma creatinine and (D) Blood urea nitrogen (BUN). All results are shown as mean and standard deviation for each timepoint. A significant decrease can be seen in the urine output and the eGFR following ischemia-reperfusion injury. Accordingly, a significant increase is noted in plasma creatinine and BUN. Data were analyzed by two-way repeated measures ANOVA with the Benjamini and Hochberg's false discovery rate (n=6). *p < 0.05 vs Baseline; **p < 0.01 vs Baseline; ***p < 0.001 vs Baseline. Please click here to view a larger version of this figure.
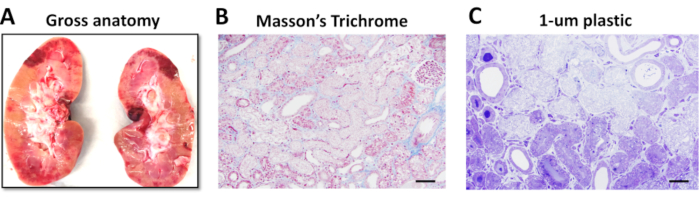
Figure 3. Gross kidney anatomy and renal tissue injury at 24 hours of reperfusion following renal ischemia-reperfusion injury. (A) Gross anatomy of the left kidney showing pale areas indicative of infarction and red hemorrhagic areas following 60 min of bilateral renal artery occlusion and 24 h of reperfusion. (B) Renal Cortex of vehicle shows extensive coagulative necrosis of primarily proximal tubules, following 60 min of ischemia and 24 h of reperfusion (Masson's Trichrome, original magnification 20x). (C) These 1 µm plastic (araldite-epon) embedded sections demonstrate in greater detail the confluent tubular necrosis consisting primarily of matrix with swelling and degenerative changes of organelles (Toluidine blue, original magnification 40x). Scale bar = 200 µm. This figure has been modified from Doulamis et al11. Please click here to view a larger version of this figure.
