Typical assay results and performance evaluations
Immunobead assays commonly provide a sigmoidal curve when evaluated over several (log) orders of magnitude, as illustrated in each of the panels presented in Figure 1. The user must experimentally define the optimal concentration range for each analyte in the multiplex to determine the full range of quantitation, ensuring to not over-sample the extremes (areas approaching the lower limit of quantitation [LLOQ] or upper limit of quantitation [ULOQ]). The actual range required for an assay, however, is dictated by the distribution of the target analytes in a biological matrix (i.e., the 'unknowns') at a given dilution factor. Further, although standard curves are typically interpreted via linear regression with a 4- or 5-parametric fit algorithm, the linear portion of a given curve typically provides the greatest confidence in quantitative accuracy with a linear (y = mx + b) model of quantitation. Matching the calibration curve to the observed values for an unknown at a given dilution factor should be the goal in quantitative assay development.
In this regard, a 7-point standard curve based on a 1:5 serial dilution series was evaluated for each of Spike S1, Nucleocapsid, and Membrane antibodies that range between 1 µg/mL and 0.000064 µg/mL for Spike S1 and Nucleocapsid and 5 µg/mL and 0.00032 µg/mL for Membrane, as shown in Figure 1.The lower limit of detection (LLOD) for each assay was defined as the lowest analyte concentration that yielded a signal distinguishable from its background. LLOD can be identified by the equation described previously8,9, LLOD = LoB + 1.645(SDlow concentration sample). LoB is the lower limit of blank, and it is the "apparent" concentration of analyte that is produced from the blank when a zero value is expected, and it can be ascertained using this equation LoB = Meanblank + 1.645(SDblank)8. Based on this method, the MFI values for the Spike S1 assay ranged from 134.38 to 20191.2, with 134.38 MFI representing 0.00024 µg/mL and defined as the LLOD. For the Membrane assay, the practical MFI range was 52.24 to 4764.9, with 52.24 MFI calculated to be 0.004885 µg/mL and assigned as the LLOD. The MFI range for the Nucleocapsid assay was 517.9 to 19666.34, with 517.9 specified as 0.00024 µg/mL, which was the LLOD. The upper limit of detection (ULOD) is defined as the concentration of analyte after which the change in MFI is no longer linear, and the signal response is saturated. It should be noted that the full sigmoidal character of these curves is not observable for the standards tested, with the exception to the Nucleocapsid curve. However, given the observed MFI values for all unknowns assayed to date (at a 1:500 dilution) are within the presented curve range for each analyte and are easily quantified using a 4- or 5- parametric fit via linear regression.
Assay precision
Intra-assay precision: Four replicates of assays were performed on the same plate to assess assay precision, calculated as the %CV, or the quotient of the standard deviation and the average multiplied by 100. Standard points 2 and 5 were selected for these tabulations, with values cataloged in Table 2. The typical acceptable upper limit threshold for %CV values are ≤20%, which was observed for these data, with the exception to that for standard 2 of Membrane IgG, which likely results from background levels and can be rectified by eliminating outlying values (data not shown). It should be noted that an apparent instability to read value was observed for Membrane assays where the MFI values were <200, most commonly in the case of IgA and IgM isotypes.
Inter-assay precision: Three distinct batches of bead sets were prepared for each assay and tested, as defined for Intra-assay precision (above and as seen in Figure 1). Inter-assay variability was assessed by calculating the %CV from the average results for each of three batches, as shown in Table 3. Again, the upper limit threshold for an acceptable %CV is set at ≤20%, which exists for all conditions tested (with a similar effect with standard 2 of Membrane IgG, as seen above). It should be noted that batch-to-batch variability in net MFI values is commonly observed within multiple batches of the same immunoreagents during custom assay development. The use of a calibration curve erected from a commercially-obtained anti-target antibody (e.g., rabbit anti-Spike S1) followed by an anti-species detection antibody can provide consistency in the analytical results and permit comparisons between multiple batches at different periods of time.
Inter-assay precision with human samples: The evaluation of inter-assay precision was repeated with human plasma samples (n = 5) collected within a month of first-reported symptoms for a SARS-CoV-2 infection; accomplished with three distinct batches of assays (i.e., different preparations of the bead sets). These results are depicted in Table 4 and demonstrate precision with a %CV value with the typical upper threshold limit value of ≤20%. The averaged %CV values for the Spike S1, Nucleocapsid and Membrane IgG titers were calculated to be 9.9% (range 2.6%-18%), 11.0% (range 3.5%-24.4%), and 7.6% (range 3.2%-12.9%), respectively. Similar observations were made with the IgM and IgA titers of these three analytes, all providing %CV values <20%. The only exception to this was Subject 5 IgM titers for the Membrane protein, which was subsequently excluded as an outlier. The precision values for the human subject evaluations are consistent with those seen above for the rabbit antibodies, which suggests these assays may be readily reconfigured to evaluate titers of the antigens in multiple species with little impact on assay precision. As noted above, there was an apparent instability to read values observed for Membrane assays where the MFI values were <200, most commonly in the case of IgA and IgM isotypes.
Primary antibody concentration optimization
The analyte 'capture time' was evaluated with the antigen-conjugated beads, and the antibodies in the plasma specimens or in the standards were tested by modifying the length of the primary incubation (30 min, 1 h, 2 h, and 4 h). The difference in the average MFI is presented as the quotient of a specific incubation and the maximum incubation time, termed % Max., in Figure 2, between a 30 min incubation (minimum duration) and a 4 h incubation (maximum duration). Values at 120 min were optimal for IgG titers for the Spike S1, the Membrane, and the Nucleocapsid antibodies, indicating a fast-primary antibody binding kinetics, allowing flexibility to increase assay throughput. However, slower kinetics were observed for the IgA and IgM (data not shown) isotypes, demonstrating peak capture levels at the 4 h time point, as shown in Figure 2. Overall, there is a balance between approaching assay saturation and the practical time expediency for running each assay when in production (to maximize throughput). With this, suitable signals for quantitative purposes at minimal incubation times of 30 min for IgG, 60 min for IgM, and 120 min for IgA were observed in these findings.
Secondary antibody concentration optimization
Five concentrations of secondary antibodies (goat anti-human IgG, PE-conjugated; goat anti-human IgA, PE-conjugated; goat anti-human IgM, SB-conjugated) were tested (0.5, 1, 2, 4, and 8 µg/mL). All antibodies revealed wide ranges of signal, with no obvious signal saturation in any condition, thereby ensuring a linear measurement for any of the concentrations. As an example, the average signal generated from the Spike S1 assay using goat anti-human IgM, SB-conjugated at 0.5 µg/mL was 13.2% of the MFI generated from the maximum signal (8 µg/mL), whereas MFI generated from 4 µg/mL was 73.3% of the MFI manifested at the maximum signal. Details of the range of signals from the other Spike S1 antibody isotypes, the Membrane antibodies, and the Nucleocapsid antibodies are included in Table 5 and Figure 3. As a practical point, the primary impact between the optimal secondary antibody concentration and the previously stated 4 µg/mL secondary antibody concentration is reflected in terms of assay sensitivity and assay cost. That is, an 8 µg/mL secondary antibody concentration may be desirable for application with low antibody titers or low amounts of valuable sample, but the cost associated with these assays would be considerably higher than the use of the previously defined 4 µg/mL concentration. Inversely, instances in which high antibody titers were to be observed (such as individuals that have experienced Covid-19 vaccinations or with non-limiting amounts of sera) would see a cost-benefit through the application of the lower quantities of secondary antibodies (e.g., 1 µg/mL).
Secondary antibody incubation optimization
The potential influence of the duration of the secondary antibody incubation was also investigated by modifying the length of the incubation (15, 30, 60, and 120 min). Generally, the difference in the average MFI as presented as the quotient of a specific incubation and the maximum incubation time, termed %Max, between a 15 min incubation (minimum duration) and a 120 min incubation (maximum duration) did not exceed 30%, 55%, and 50% for the Spike S1, the Membrane, and the Nucleocapsid antibodies, respectively, indicating a fast kinetic step in secondary antibody binding and a means to increase assay throughput. Table 6 includes details on signal changes for all incubation times. Illustrations of the observed signals from different incubations of this analysis are shown in Figure 4.
Dual-channel performance and specificity
For each analyte, a single reporter format run (IgG-PE only, IgA-PE only, or IgM-SB only) was compared to the signal generated for the same analyte when it was run in a dual-reporter format (e.g., Spike S1 IgG-PE only versus Spike S1 IgG-PE in combination with Spike S1 IgM-SB in the dual-reporter format). Assay precision (expressed as %CV) for the signals created in the two formats were used to analyze the relationship in the findings of this experiment. The %CV values of the Spike S1 assays were 6.19%, 16.4%, and 23% for IgM, IgG, and IgA, respectively. For the Membrane assay, the %CV values were 3.3%, 7.9%, and 16.4% for IgM, IgG, and IgA, respectively. Finally, the Nucleocapsid assay provided %CV values at 8.7%, 10.3%, and 24.2% for IgM, IgG, and IgA, respectively. The precision values observed for the IgM and IgA isotypes suggest a longer incubation time may confer superior assay results due to the known binding kinetic differences across these classes of immunoglobulins. Figure 4 shows the agreement between the formats of different concentrations of secondary antibodies.
To confirm the specificity of reporter channels, a single reporter channel was tested at one time while the other channel was assigned as a blank to inquire about the non-specific signal (bleeding effect). These findings indicate there is negligible cross-signal contamination between the two reporter channels, given the high specificity across the spectrum of conditions. These findings are illustrated in Figure 5. Overall, we observed a 6.45% interference across channel 1 to channel 2. However, when the magnitude of the signals was accounted for, we observed the following potential interference levels in dual reporter mode: Spike IgG/ IgM at 71.98%, Spike IgA/ IgM at 28.11%; Membrane IgG/ IgM at 7.41%, Membrane IgA/ IgM at 134.61%; and Nucleocapsid IgG/ IgM at 146.03%, Nucleocapsid IgA/ IgM at 112.13%. In the specified configuration, this would necessitate measurement of Spike IgM in combination with the IgA isotype, Membrane IgM with the IgM isotype, and nucleocapsid measurements not performed in a dual-channel format. This finding may necessitate exploration of the inversion of the labeling strategy whereby IgA and IgG be measured in channel 2 and IgM in Channel 1.
Evaluation of seroconversion events following Covid-19 vaccination
Seroconversion was monitored in four subjects upon assessment of IgA, IgM, and IgG with the Spike S1 assay at time points ranging from pre-vaccination to four months after completion of the Covid-19 vaccination series. Measurements were accomplished in dual channel mode (IgG/ IgM and IgA/ IgM, with IgM values averaged). All subjects received the vaccine as a 2-stage immunization, per standard practice, with a 21-day interval between the first and second doses. Plots of each subject's immune response are shown in Figure 6A–C. Immune response values for the Nucleocapsid and Membrane antigens were observed at background levels for all immunoglobulins evaluated (data not shown), which was consistent with the subjects having no documented prior SARS-CoV-2 infection in the time prior to vaccination. Overall, the observed Spike S1 IgA and IgM values were approximately 40-fold lower than the IgG isotype titers, with peak titers being cresting as soon as 14 days for both IgM and IgG isotypes and the IgA isotype reaching peak titers between the time of the second dose (day 0) and 14 days post second dose, depending on the subject. Notably, the Spike S1 IgG titers start decaying during the course of the four months following completion of vaccination at a highly variable rate, in a subject-dependent manner.
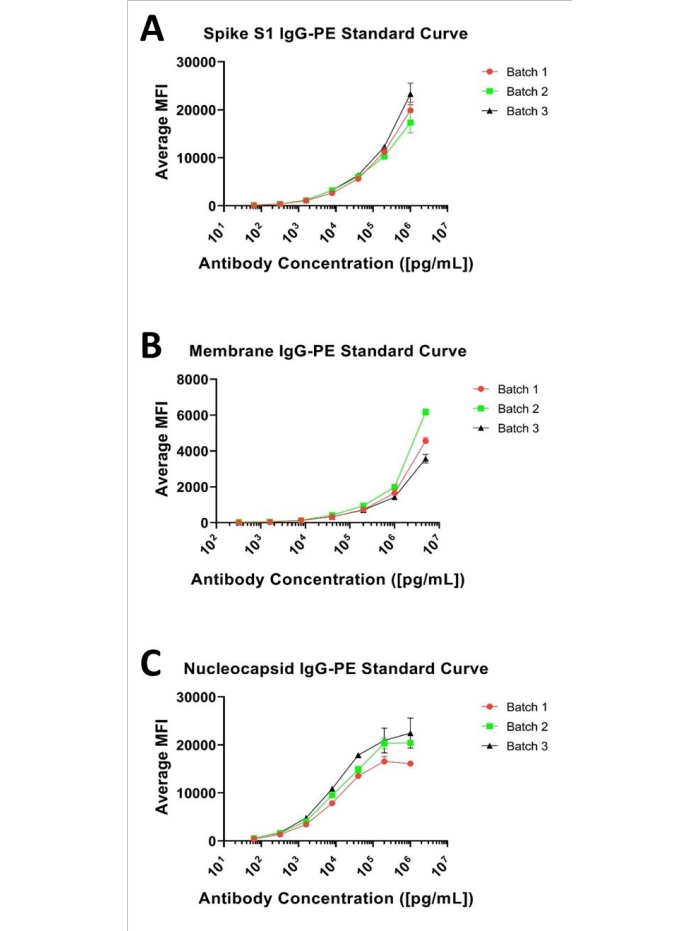
Figure 1: Representative 3-plex standard curves. Representative standard curves for the three analytes; presented as a 7-point, 1:5 serial dilution curve starting at (A) 1 µg/mL for Spike S1, (B) 5 µg/mL for Membrane, and (C) 1 µg/mL for Nucleocapsid and antibodies. Please click here to view a larger version of this figure.
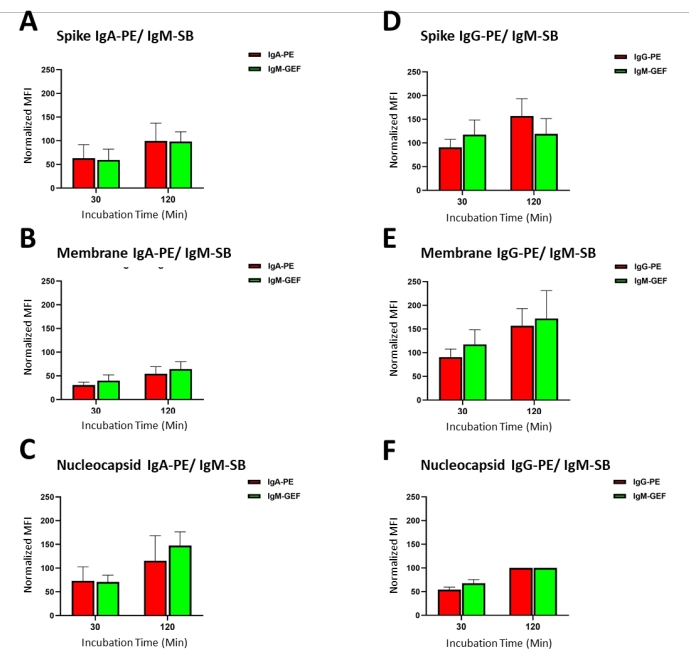
Figure 2: Primary antibody/sample incubation time optimization: The average MFI signal produced from different incubation times of primary antibody/samples (antibody capture) ranging from 30 min to 4 h for standards 1-7 (as indicated in Table 1). Please click here to view a larger version of this figure.
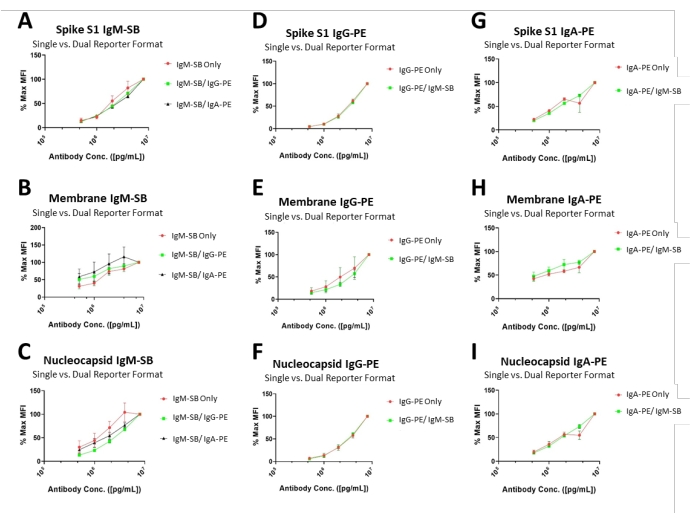
Figure 3: Secondary antibody concentration optimizations and dual-channel performance. Curves illustrate the average MFI (normalized to the highest recorded value in the series) produced from tested secondary antibody concentrations, ranging from 0.5-8 µg/mL. Each instance was performed both as a single- and dual-channel assay to appreciate differences in the experimental format. Please click here to view a larger version of this figure.
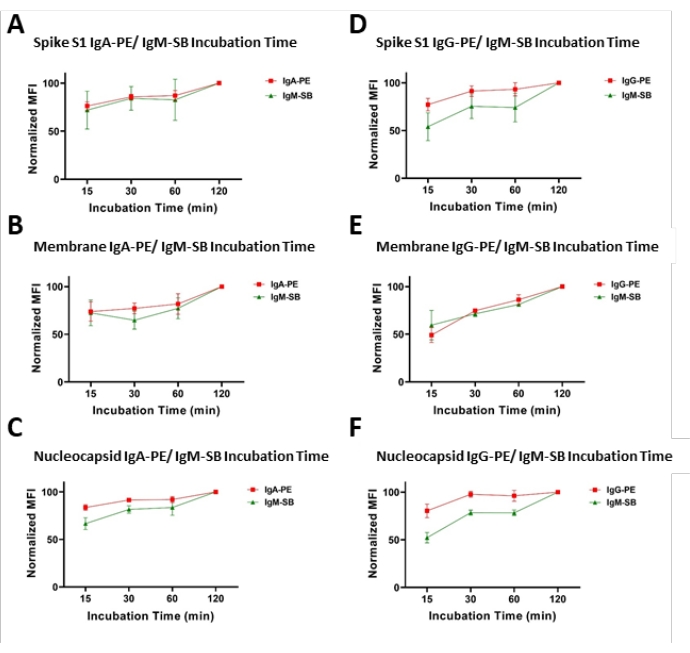
Figure 4: Secondary antibodies incubation time optimization, dual-channel format. Representative plots of observed MFI values (normalized to the highest recorded value in the series) with respect to time of incubation with secondary antibodies. Experiments were performed as dual-channel assays as (A–C) IgA/IgM or (D–F) IgG/IgM combinations. Please click here to view a larger version of this figure.
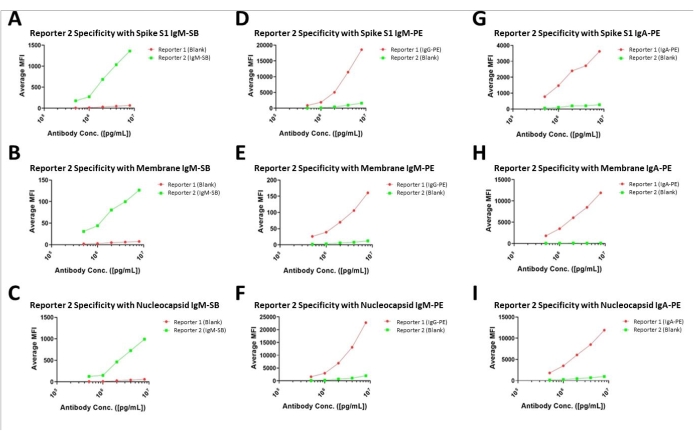
Figure 5: Specificity assessments for dual-channel assays. Assay results of the dual-channel assay format with one of each combination designated as the blank to illustrate the lack of cross-channel fluorescent or interference. Please click here to view a larger version of this figure.
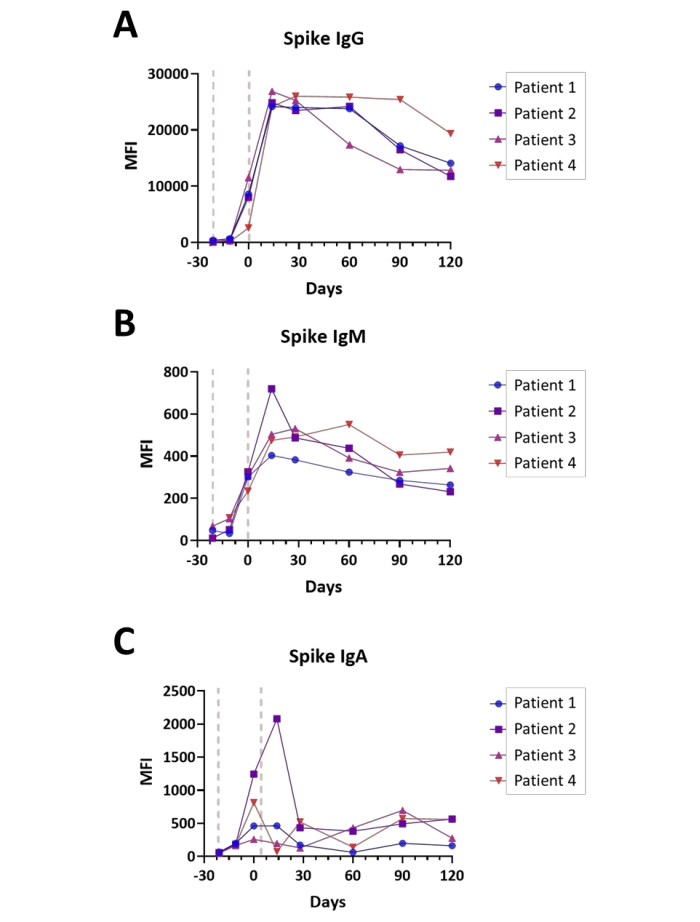
Figure 6: Illustration of seroconversion following Covid-19 vaccination. Plots illustrating the relative titers of (A) IgG, (B) IgM, and (C) IgA antibodies for the Spike S1 antigen during the course of Covid-19 vaccination (Pre-vaccination – 4 months post-completion); time is shown in days relative to completion of the vaccination series; general points of the vaccine administration are indicated (red lines). Experiments were performed in dual channel mode, as described in the Protocol. Please click here to view a larger version of this figure.
| Standard Number | Dilution series | Anti-Spike S1 or N (µg/mL) | Anti-Membrane (µg/mL) |
| Blank | Blank | – | – |
| 1 | STD7 1:1 | 1 | 5 |
| 2 | STD6 1:5 | 0.2 | 1 |
| 3 | STD5 1:25 | 0.04 | 0.2 |
| 4 | STD4 1:125 | 0.008 | 0.04 |
| 5 | STD3 1:625 | 0.0016 | 0.008 |
| 6 | STD2 1:3125 | 0.00032 | 0.0016 |
| 7 | STD1 1:15625 | 0.000064 | 0.00032 |
Table 1: Dilution series for standard curves: Table of dilution factors used for the standard curves for the IgG serotype; presented as a 7-point, 1:5 serial dilution curve starting at 1 µg/mL for α-Spike S1 and α-Nucleocapsid and 5 µg/mL for α-Membrane antibodies.
| Analyte | Sample | Rep 1 | Rep 2 | Rep 3 | Rep 4 | Ave | SD | %CV |
| Spike S1 | STD2 | 369.4 | 356.9 | 295.2 | 271.5 | 323.3 | 47.4 | 14.6 |
| STD5 | 3869.1 | 3437 | 3970.2 | 4240.7 | 3879.3 | 334 | 8.6 | |
| Membrane | STD2 | 40.6 | 37.7 | 49.9 | 27.8 | 39 | 9.1 | 23.3 |
| STD5 | 733.2 | 731.3 | 724 | 678.1 | 716.7 | 26 | 3.6 | |
| Nucleocapsid | STD2 | 1746.7 | 1790.8 | 1577.3 | 1664.8 | 1694.9 | 94.2 | 5.6 |
| STD5 | 15598.1 | 14735.5 | 18369.5 | 17408.5 | 16527.9 | 1657.7 | 10 |
Table 2: Intra-assay precision: Percent coefficient of variance (%CV) calculated from four replicates of standard antibody mixtures at standard 2 (STD2) and standard 5 (STD5) with a single assay batch in the same experiment. Values provided for replicates and averages represent the observed MFI values.
| Analyte | Sample | Batch 1 | Batch 2 | Batch3 | Ave | SD | %CV |
| Spike S1 | STD2 | 383.2 | 424.4 | 379.9 | 395.8 | 24.8 | 6.3 |
| STD5 | 5639.7 | 6062.5 | 6384.3 | 6028.8 | 373.4 | 6.2 | |
| Membrane | STD2 | 39.1 | 58.5 | 59.1 | 52.2 | 11.4 | 21.8 |
| STD5 | 732.3 | 941.4 | 701.1 | 791.6 | 130.7 | 16.5 | |
| Nucleocapsid | STD2 | 1342.6 | 1621 | 1718.2 | 1560.6 | 195 | 12.5 |
| STD5 | 13543.9 | 14843.2 | 17883.4 | 15423.5 | 2227.2 | 14.4 |
Table 3: Inter-assay precision with standard samples: Percent coefficient of variance (%CV) calculated from three distinct batches of assays, evaluated at standard 2 and standard 5 in the same experiment. Values provided for replicates and averages represent the observed MFI values.
| IgG-PE | IgM-SB | IgA-PE | |||||
| Ave. MFI | %CV | Ave. MFI | %CV | Ave. MFI | %CV | ||
| Spike S1 | Subject 1 | 8002.3 | 17.7 | 1949.5 | 1.3 | 2045.8 | 5.5 |
| Subject 2 | 19155.8 | 7.3 | 918.6 | 4.1 | 1684.5 | 3.9 | |
| Subject 3 | 17865.6 | 18.0 | 549.4 | 3.8 | 961.3 | 8.1 | |
| Subject 4 | 11901.1 | 2.6 | 1603 | 4.8 | 8736.4 | 5.5 | |
| Subject 5 | 9801.8 | 4.0 | 1014.1 | 3.0 | 2747.6 | 9.3 | |
| Nucleocapsid | Subject 1 | 15097.8 | 11.3 | 1049.7 | 9.9 | 5276.5 | 3.9 |
| Subject 2 | 15204.3 | 12.1 | 265.9 | 5.2 | 6761.3 | 11.9 | |
| Subject 3 | 18471.7 | 24.4 | 329.1 | 4.5 | 14308 | 2.9 | |
| Subject 4 | 16424.7 | 3.5 | 2418.1 | 0.1 | 4234.7 | 4.2 | |
| Subject 5 | 13344.9 | 3.6 | 225.6 | 10.0 | 13436.5 | 9.7 | |
| Membrane | Subject 1 | 514.6 | 8.6 | 180.6 | 14.0 | 141.2 | 9.8 |
| Subject 2 | 196.8 | 5.2 | 57 | 20.7 | 55.5 | 13.0 | |
| Subject 3 | 553.7 | 12.9 | 54.5 | 21.2 | 191.2 | 18.6 | |
| Subject 4 | 377.9 | 3.2 | 68.1 | 22.1 | 62 | 2.3 | |
| Subject 5 | 325.4 | 8.2 | 11.4 | 91.6 | 74.6 | 20.8 |
Table 4: Inter-assay precision with human samples: Average percent coefficient of variance (%CV) calculated from three batches of assays tested with plasma samples (diluted 500-fold) from five human subjects with SARS-CoV-2 infections.
| Spike S1 | Membrane | Nucleocapsid | |||||
| µg/mL | Ave. MFI | % Max. | Ave. MFI | % Max. | Ave. MFI | % Max. | |
| IgM | 0.5 | 186 | 13.2 | 32 | 25.2 | 132.7 | 13.6 |
| 1 | 304.2 | 21.6 | 45.8 | 36 | 194.4 | 19.9 | |
| 2 | 664.5 | 47.2 | 78.8 | 61.9 | 458.2 | 47 | |
| 4 | 1032.1 | 73.3 | 101.3 | 79.6 | 707.8 | 72.6 | |
| 8 | 1407.1 | 100 | 127.2 | 100 | 975 | 100 | |
| IgG | 0.5 | 809.7 | 4.9 | 27.5 | 15 | 1355.6 | 6.3 |
| 1 | 1696.9 | 10.2 | 40.6 | 22.2 | 2782.1 | 13 | |
| 2 | 4543.8 | 27.3 | 68.3 | 37.3 | 6661.2 | 31.2 | |
| 4 | 10003.5 | 60 | 110.7 | 60.5 | 12605.6 | 59 | |
| 8 | 16662.8 | 100 | 182.9 | 100 | 21360.6 | 100 | |
| IgA | 0.5 | 797.4 | 19.3 | 31.1 | 47.2 | 2056.5 | 16.1 |
| 1 | 1529.5 | 37 | 41.4 | 62.8 | 3869 | 30.4 | |
| 2 | 2261.3 | 54.7 | 48.6 | 73.3 | 6648.9 | 52.2 | |
| 4 | 2320.4 | 56.2 | 48.3 | 73.2 | 6548.1 | 51.4 | |
| 8 | 4132.2 | 100 | 65.9 | 100 | 12744.8 | 100 | |
Table 5: Secondary antibody concentration optimization: The average MFI signal produced from different concentrations of secondary antibodies ranging from 0.5 µg/mL to 8 µg/mL. The value of each signal is also presented as a percentage of the signal at 8 µg/mL ("Max.") to demonstrate relative signal magnitude.
| Spike S1 | Membrane | Nucleocapsid | |||||
| Incubation time (min.) | Ave. MFI | % Max. | Ave. MFI | % Max. | Ave. MFI | % Max. | |
| IgM | 15 | 1185 | 72.2 | 40.4 | 48.9 | 609.5 | 53.3 |
| 30 | 1416.6 | 86.3 | 58.4 | 70.7 | 894.2 | 78.2 | |
| 60 | 1324.8 | 80.7 | 73.6 | 89.1 | 945.6 | 82.7 | |
| 120 | 1641.2 | 100 | 82.6 | 100 | 1143.2 | 100 | |
| IgG | 15 | 12917.6 | 80.5 | 244.4 | 44.9 | 15429.8 | 80.8 |
| 30 | 14915.4 | 92.9 | 434.7 | 79.9 | 18797 | 98.5 | |
| 60 | 15340.3 | 95.6 | 421.4 | 77.5 | 18694.4 | 97.9 | |
| 120 | 16050.3 | 100 | 544 | 100 | 19085.8 | 100 | |
| IgA | 15 | 3141.9 | 78.2 | 75 | 66.8 | 9103 | 86.6 |
| 30 | 3569.1 | 88.8 | 83.9 | 74.8 | 9563.8 | 91 | |
| 60 | 3539.1 | 88 | 86 | 76.6 | 9555.7 | 90.9 | |
| 120 | 4020 | 100 | 112.2 | 100 | 10512.9 | 100 |
Table 6: Secondary antibody incubation time optimization: The average MFI signal produced from different incubation times of secondary antibodies ranging from 15 min to 120 min. The value of each signal is also represented as a percentage of the signal at 120 min ("Max.") to demonstrate relative signal magnitude.
