To assess the feasibility and stability of this experimental method, the same procedure was performed on ten mice, and observations were made regarding mortality, changes in wound size, body weight, and histologic analysis. The mice were euthanized on day 7.
The procedure exhibited a low mortality rate. The ophthalmologic cautery and germinator, depicted in Figure 1A–C, were the key instruments utilized in this experiment. The ONF model was created according to the provided protocol. Among the ten mice operated on, only one expired on the 7th day post-operation. The overall mortality rate throughout the experiment was approximately 10%.
The results revealed notable variability in the size of the ONF generated using the described method. On the day of surgery, all mice exhibited oval-shaped wounds measuring 2.0 mm in length and 1.5 mm in width. When assessing ONF formation on the 7th day after surgery, a significant variation in ONF size was observed (P = 0.0085) (Figure 5A,B).
The presence of ONF can result in complications such as food reflux and eating difficulties, potentially leading to changes in weight. Therefore, the body weight of the mice was also taken into account. The mice were weighed on the day of surgery (day 1) and on the 7th day (day 7) when ONF formation was examined. A significant reduction in weight was observed on day 7 compared to day 1 (P < 0.001) (Figure 6A,B). The loss of their body weight was 25.16%.
For histologic analysis, both the wound and normal tissue were harvested from the mice on day 7. Isolated palates were used as samples for histology sectioning. They were placed in tissue embedding boxes and fixed using 4% paraformaldehyde and 10% formic acid decalcification reagent. The tissues were then embedded in paraffin, sectioned into 7 µm slices along coronal planes, and stained with hematoxylin and eosin (H&E). Histological analysis of the ONF revealed loss of hard palate mucosa, denuded bone, and ONF formation (Figure 7). Histology of the lungs was performed, and no abnormalities were detected between normal and ONF mice.
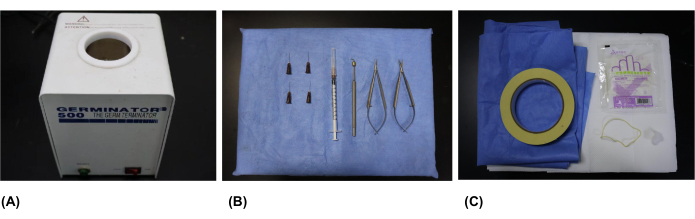
Figure 1: Surgical instruments and supplies. (A) The germinator used for heating the ophthalmologic cautery. (B) Surgical instruments: ophthalmologic cautery, microsurgical scissors, microsurgical tweezers, syringes, and needles (26 g x 0.63 inch). (C) Surgical supplies: surgical drapes, sterile gloves, sterile cotton, sterile sheets, sterile metal foil, foam board, rubber bands, and tape. Please click here to view a larger version of this figure.
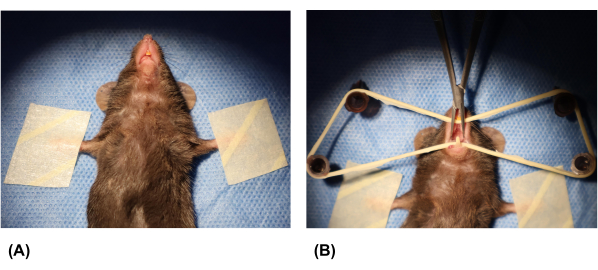
Figure 2: Fixation of the mouse and opening of the oral cavity. (A) The forelimbs of the mouse were taped to secure it. (B) Syringe needles were inserted into the foam board, and a rubber band was placed over the needles. The mouse's oral cavity was opened using a rubber band and microsurgical tweezers. Please click here to view a larger version of this figure.
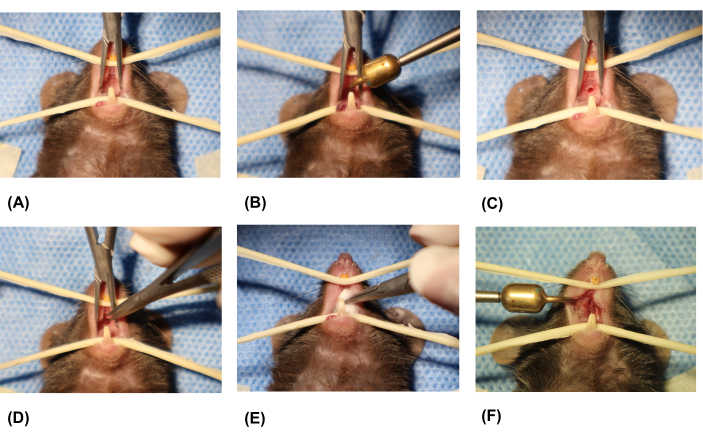
Figure 3: Creation of the oronasal fistula. (A) Exposing the oral cavity. (B) Placing the tip of the ophthalmologic cautery on the midline portion of the hard palate. (C) Removing the ophthalmologic cautery. (D) Removing excess soft tissue around the wound using microsurgical scissors. (E) Stopping bleeding using sterile cotton. (F) Final formed palatal wound. Please click here to view a larger version of this figure.
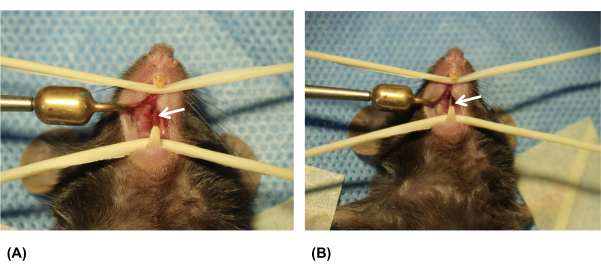
Figure 4: Examination of the palatal wound on the 7th day after surgery. (A) Palatal wound on day 1. (B) Palatal wound on day 7. White arrows indicate the oronasal fistula (ONF). Please click here to view a larger version of this figure.
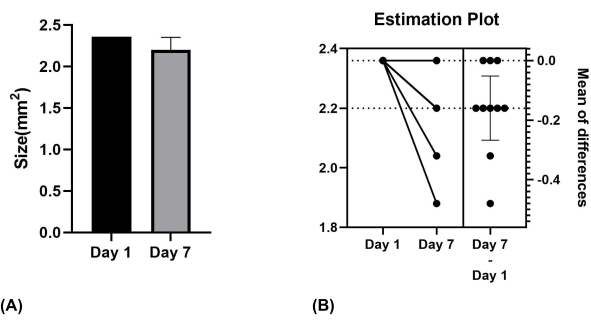
Figure 5: Size of the palatal wound on Day 1 and Day 7. (A) Mean values for mice on days 1 and 7. (B) Significant difference verified using paired samples t-test. Please click here to view a larger version of this figure.
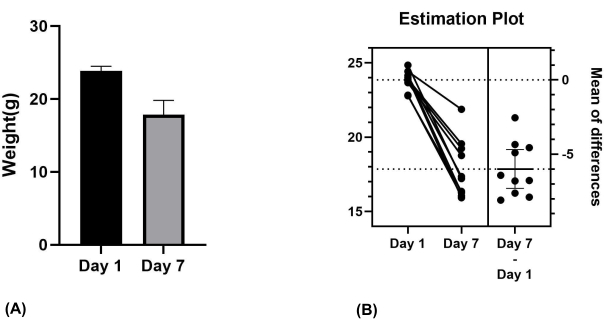
Figure 6: Weight of the mice on day 1 and day 7. (A) Mean values for mice on day 1 and day 7. (B) Significant difference verified using paired samples t-test. Please click here to view a larger version of this figure.
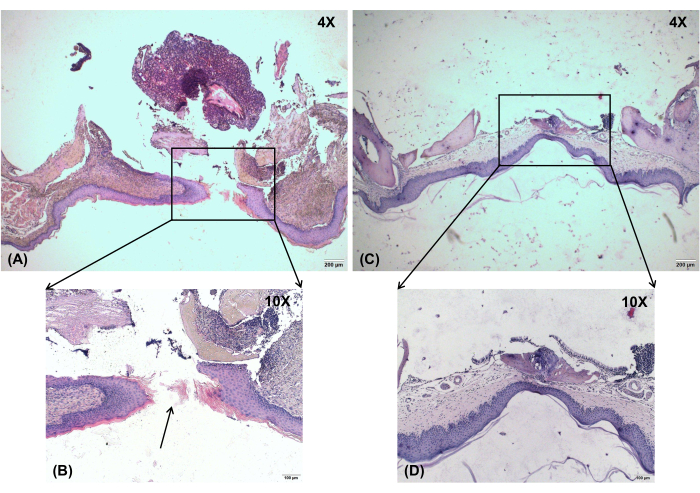
Figure 7: Histological observation. Histological analysis of the ONF shows loss of hard palate mucosa, denuded bone, and ONF formation. (A) Oronasal fistula on day 7, magnification: 4x. (B) Oronasal fistula on day 7, magnification: 10x. (C) No-injury control, magnification: 4x. (D) No-injury control, magnification: 10x. Black arrow shows the location of the ONF. Scale bars: A,C = 200 µm; B,D = 100 µm. Please click here to view a larger version of this figure.
