The AACP was applied to one group of children11: 155 normally developing infants and toddlers (5 to 36 months old, based on gestational age). In a previously published study, the grating acuity results obtained by the AACP were compared with those obtained by TACII. The results obtained by these two procedures are significantly correlated (r153 = 0.83, p < 0.001). Only 10.32% (16 of 155) of the children's results differed by more than one octave. Among them, eight children were 5-7 months old. Of these 16 children, three had visual acuity results obtained by the AACP that were 1.5-2 octaves over those obtained by TACII. The other 13 children had AACP visual acuity 1.5-2 octaves below TACII visual acuity.
The grating acuity measured by the AACP gradually increased as infant age increased. Figure 5 shows the change in grating acuity measured by the AACP with the change in age in months. From 6 to 12 months, the grating acuity increased by nearly 0.5 octaves. From 12 to 24 months, the grating acuity increased by almost one octave. From 24 to 36 months, the grating acuity increased by nearly 1.5 octaves. The trend of acuity development in this study is consistent with the results of acuity measured by TACII in previous studies12. It is also consistent with the acuity development measured by TACII in the same group of infants11.
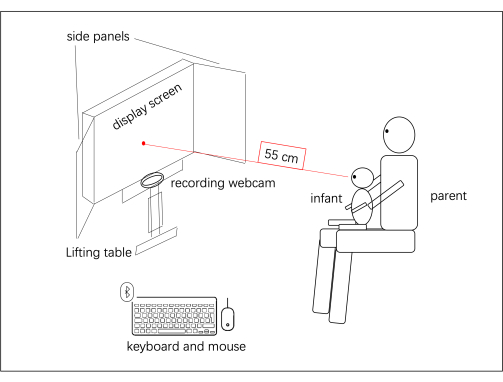
Figure 1: AACP apparatus. The AACP components and the spatial arrangement of their setup in the test room are shown. The infant was seated on a parent's lap and viewed the stimuli binocularly at a distance of 55 cm. Please click here to view a larger version of this figure.
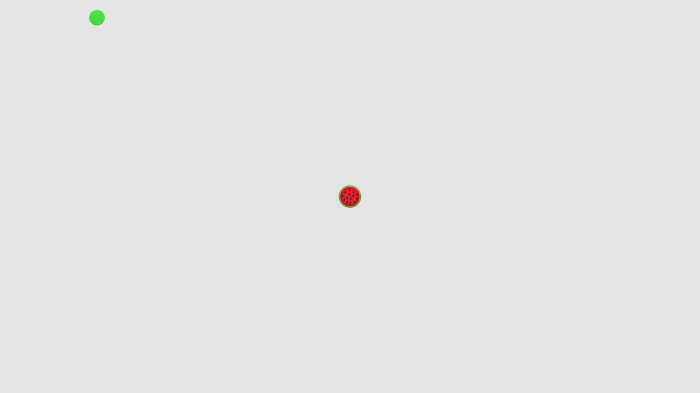
Figure 2: Cartoon stimulus in the calibration procedure. The cartoon stimulus is a GIF image with background music. The stimulus attracts visual attention. When the child's gaze falls within the image area, the dot changes from red to green, and the calibration procedure is performed. This figure has been modified with permission from Wen et al.11. Please click here to view a larger version of this figure.
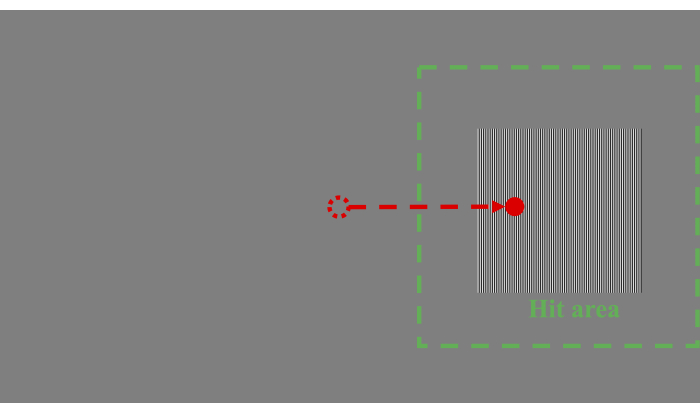
Figure 3: Grating stimulus in the testing procedure. The grating stimulus is a grating of vertical black-and-white stripes presented on a uniform gray background. The gaze point of the participant moving from the center to the green square indicates that the participant has watched the target, which means a "hit". The gaze point of the participant moving from the center to the empty area indicates that the participant did not watch the target, which means a "miss". The green square area has a half-side length based on the distance from the center of the stimulus to the side of the screen (i.e., from the center of the stimulus to the left edge of the screen in this figure). This figure has been modified with permission from Wen et al.11. Please click here to view a larger version of this figure.
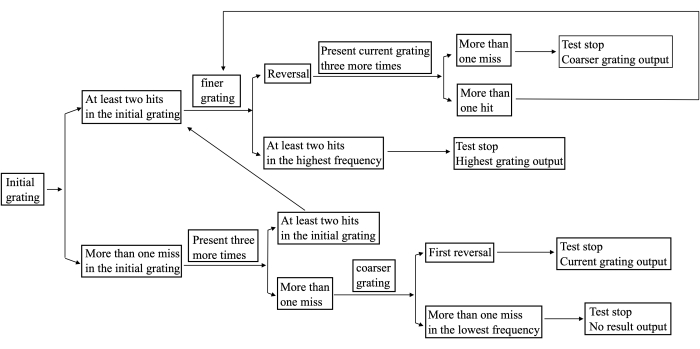
Figure 4: The protocol used in the AACP procedure. This figure has been modified with permission from Wen et al.11. Please click here to view a larger version of this figure.
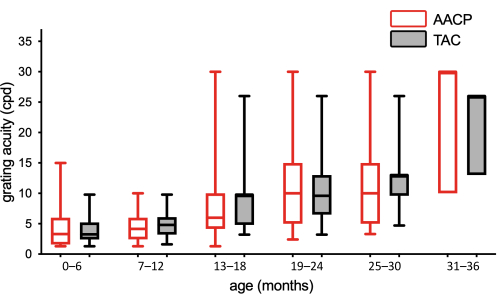
Figure 5: Box plots of grating acuities plotted against age (N = 155). White boxes with red lines and gray boxes with black lines are grating acuities of the AACP and TACII11, respectively, for every 6 months of age. Please click here to view a larger version of this figure.
| Criterion | Verify that the gaze signal: | |||
| Hit | remained in the target area continuously for more than 400 ms of the 1,000 ms target presentation. | |||
| Miss | (1) did not enter the target area within a time window of 1,000 ms. (2) remained in the target area less than 400 ms. | |||
Table 1: Criteria to establish whether a stimulus has been seen.
