Kim et al. demonstrated a more superior effect of TMS with neuronavigational system guidance compared to the non-navigated conventional method by less dispersion of stimulus and more focal stimulation to the right M1 area,8 as shown in Figure 9. Further evidence to support incorporating the neuronavigational system with TMS is demonstrated by a randomized crossover experiment to induce virtual aphasia in healthy subjects by targeting Brodmann area 44 and 45 for nTMS and F3 of the International 10-20 EEG system for cTMS.9
Kim et al. compared cTMS and nTMS in 16 healthy subjects by following measures; reaction time for a picture naming task measured before and after each session of stimulation, the mean Talairach space coordinates of localization of stimulation, and the error range relative to the target (Figures 10–12). Figure 10 shows only the nTMS induced a significant delay in reaction time compared with baseline, and greater consistency of localization of stimulation with the target in demonstrated in Figure 11. Figure 12 shows a narrower error range relative to the target for the nTMS compared with that of cTMS.
These significant differences in the nTMS group were induced by the high precision of the TMS pulse delivery to the intended target by narrowing the distance between the target and the coil when guided by neuronavigation, thereby producing more significant results compared to those of the conventional method. Exact placement of the coil on the target is absolutely critical for producing clinically effective results. Above results support use of neuronavigational guidance when applying rTMS.
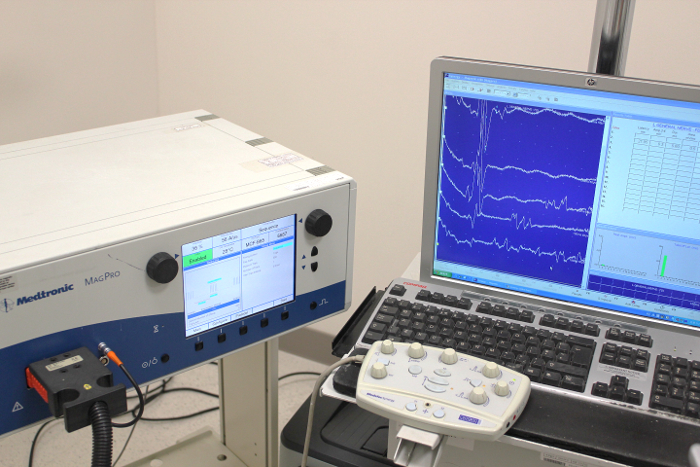
Figure 1: Transcranial Magnetic Stimulation (TMS) System and Electromyography (EMG) Machine to Acquire Resting Motor Threshold (RMT)
Right M1 area is stimulated with the active electrode on the left first dorsal interosseous muscle to determine RMT Please click here to view a larger version of this figure.
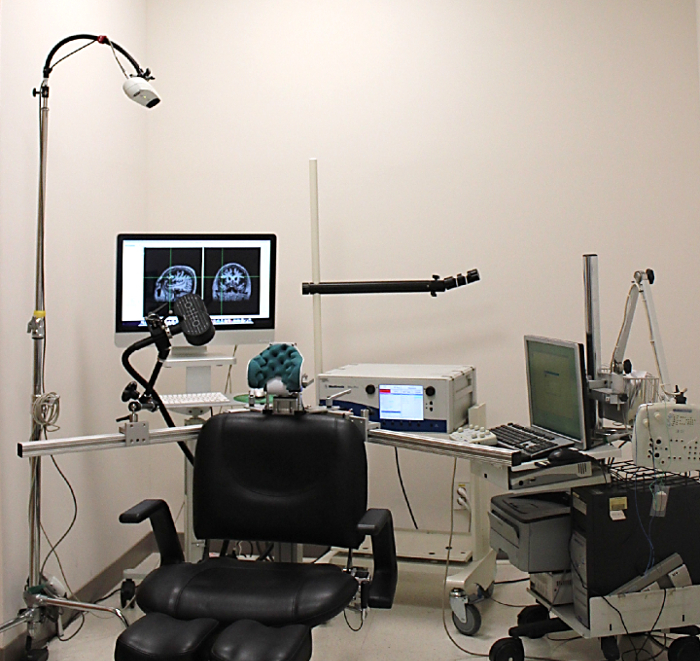
Figure 2: Equipment Setting for the Navigation System. Transcranial magnetic stimulation (TMS) chair, mobile camera, and computer screen with TMS equipment are included. Please click here to view a larger version of this figure.
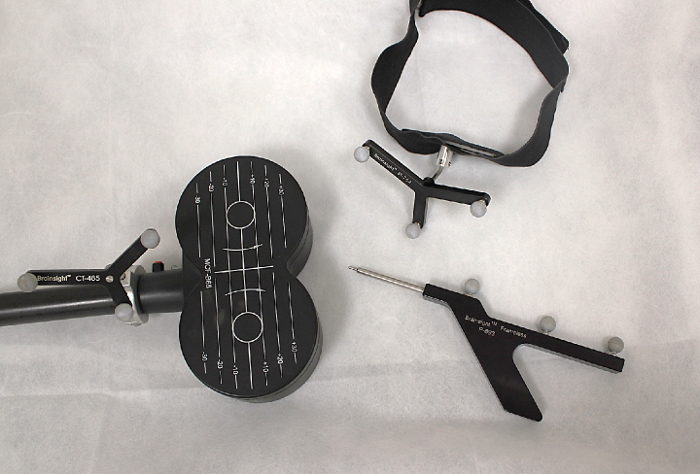
Figure 3: Preparing Materials. Picture of coil tracker, pointer, and subjective tracker. Please click here to view a larger version of this figure.
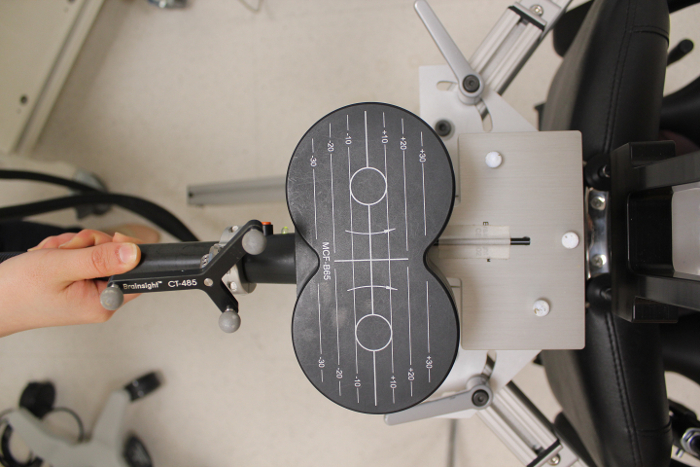
Figure 4: Calibration Block with Coil Tracker. This allows the program to detect the relative position of the transcranial Magnetic stimulation (TMS) coil. Please click here to view a larger version of this figure.
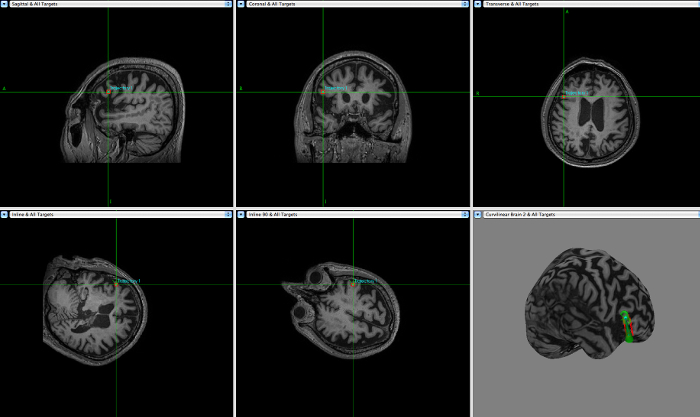
Figure 5: Reconstructed Brain Curvilinear by the Neuronavigation Program. Once the brain magnetic resonance MR images are transferred to the neuronavigation program, the brain curvilinear and skin are reconstructed using anterior commissure (AC) and posterior commissure (PC). Please click here to view a larger version of this figure.
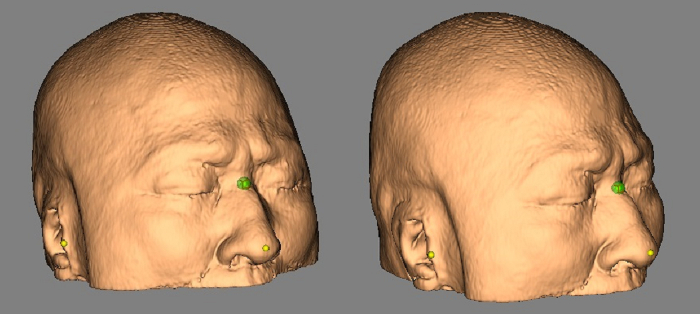
Figure 6: Anatomical Landmarks for Navigation Transcranial Magnetic Stimulation (TMS). Anatomical landmarks, nasion, nasal tip, and both tragus are marked using a pointer. Please click here to view a larger version of this figure.
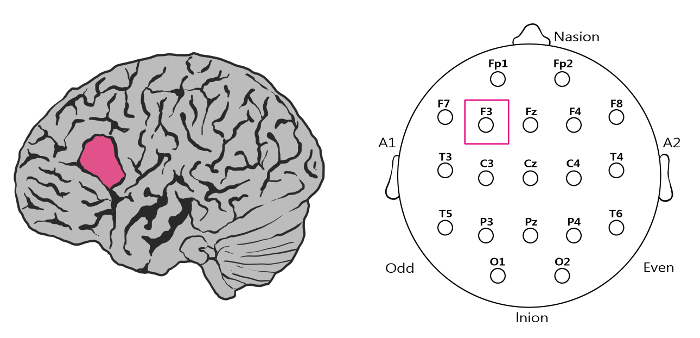
Figure 7: Transcranial Magnetic Stimulation (TMS) Mapping. Inferior frontal gyrus for the navigation-guided TMS (left) and F3 of the International 10-20 system for conventional TMS (right) are set to stimulate the target. Please click here to view a larger version of this figure.
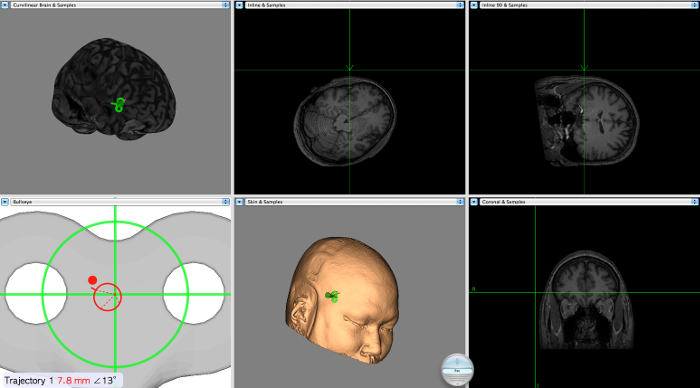
Figure 8: Neuronavigation Display during Navigation-guided Transcranial Magnetic Stimulation (nTMS). Screen displays subject's brain surface, intended target, coil, and error range. Please click here to view a larger version of this figure.
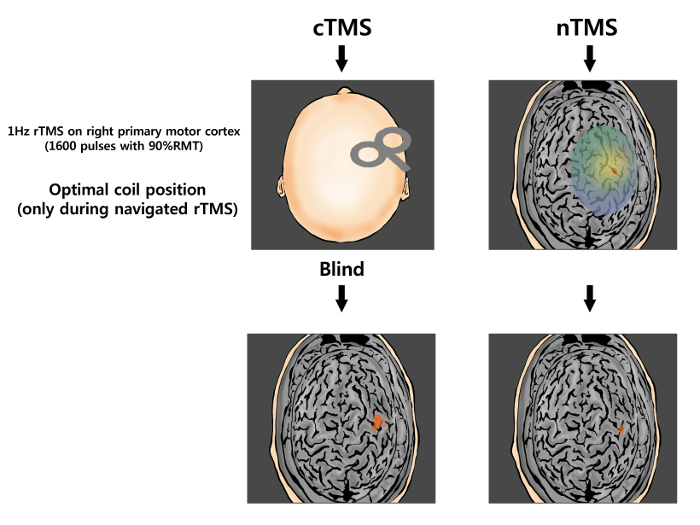
Figure 9: Less Dispersion of the Stimulus and More Focal Stimulation with the Navigation. Comparison of the non-navigated conventional method (left) with navigational guidance (right) demonstrates less dispersion of the stimulus and more focal stimulation of the right M1 area using navigation-guided transcranial magnetic stimulation (nTMS). Modified from reference9. Please click here to view a larger version of this figure.
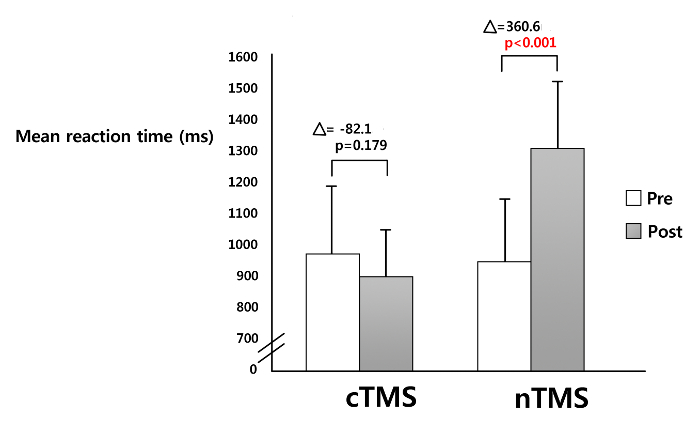
Figure 10: Comparison of the Ability to Induce Virtual Aphasia between Navigation-guided Transcranial Magnetic Stimulation (nTMS) and Conventional TMS (cTMS) in 16 Healthy Subjects. Mean picture naming time (in msec) is significantly increased (p <0.001) with nTMS whereas no change is made with cTMS (p = 0.179) Bars represent mean reaction time with corresponding standard errors. Modified from reference9. Please click here to view a larger version of this figure.
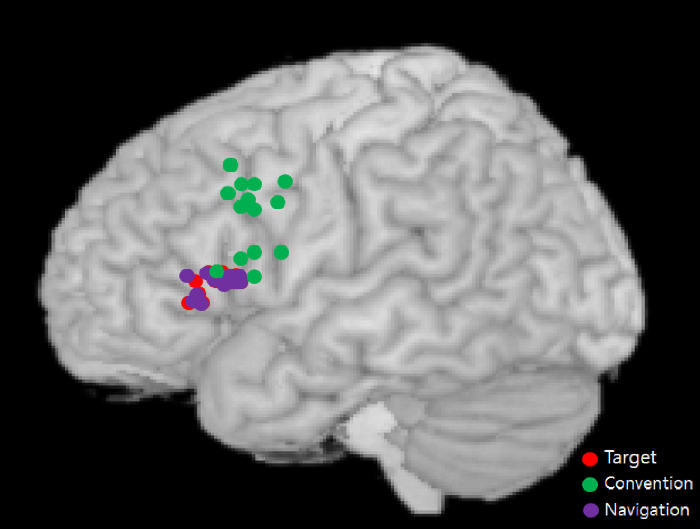
Figure 11: Drawing of Mapping Area and Stimulation (n = 16). The areas stimulated for the conventional method (green) are more widely distributed with the coordinates scattered more upward relative to the target (red) compared to those of the navigation method (purple). Modified from reference9. Please click here to view a larger version of this figure.
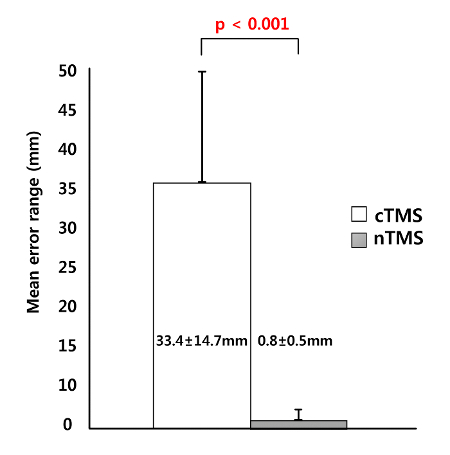
Figure 12: Mean Error Ranges for Navigation-guided Transcranial Magnetic Stimulation (nTMS) and Conventional TMS (cTMS) (n = 16). The distance from the actual stimulation site relative to the target is closer with nTMS than cTMS. The error range is narrower for nTMS than that for cTMS. Bars represent means and standard errors. Modified from reference9. Please click here to view a larger version of this figure.
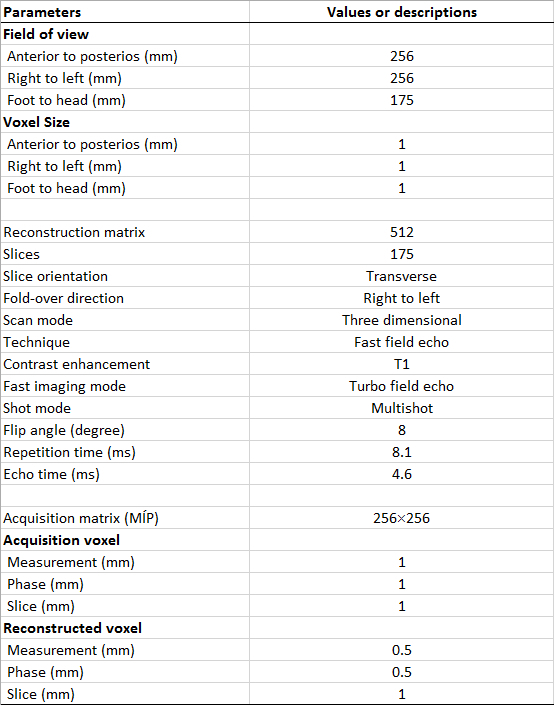
Table 1: Three-dimensional T1-weighted Magnetic Resonance Imaging (MRI) Parameters for this Study
