Recording neural activity was performed with a customized pre-amplifier using super-β input instrumentation amplifier (700 Hz – 7 kHz bandwidth and total gain of 2,000). An example of the fabricated FINE electrode with the presented protocol is shown in Figure 3. Implanting the FINE around the nerve is done by suturing the two free edges together. A demonstration of the cuff's flexibility (Figure 3B) indicates that the cuff flattens the nerve while retaining flexibility in the longitudinal direction.
In addition to the cuff flexibility in the longitudinal direction, the cuff should also be elastic to accommodate nerve swelling, especially at the early healing stages post-implantation. High pressure inside the cuff could constrict blood vessels and occlude blood flow inside the nerve. Consequently, the pressure generated inside the cuff as a result of nerve swelling should not exceed the diastolic blood pressure. Figure 4 shows the response of the assembled cuff to various pressure levels inside the cuff. As the pressure increases, the electrode expands to form a larger cross sectional area. At 67 mm Hg; the electrode expands to 1.25 times its original cross sectional area. This observation can be interpreted as if the cuff size is at least 1.2 times the initial cross sectional area of the nerve, the nerve can expand up to 1.5 its initial cross sectional area while the resulting increase in pressure inside the cuff remains under 67 mm Hg. Therefore the design criterion15, 30, 31 for a nerve cuff electrode to exhibit a cuff-to-nerve cross sectional area ratio of at least 1.5 is satisfied.
The functionality and stability of the manufactured cuff design was examined by implanting it on the sciatic nerve of a dog (Figure 5). The study was approved by CWRU IACUC and ACURO. Three parameters were periodically measured through the chronic implant duration: 1) the signal-to-noise ratio (SNR), 2) the contact impedance and 3) the number of contacts that provide viable recording. The SNR is defined as the ratio of neural activity mean power (red segment) over the mean power of baseline activity (yellow segment). 100 ms moving window was used. Throughout the 7.5-month implant duration, the SNR remained steady with a value of 5.10 ± 0.81 dB (Figure 5B).
The magnitude of contacts' impedance was measured in vivo at 1 kHz and is shown in Figure 5C. These measurements were made using the RHD2000-Series amplifier evaluation system. The impedance was observed to be stable with a mean value of 2.55 ± 0.25 kΩ (33 Trials, 16 contacts (N= 528)). Finally, the number of contacts that became inactive over time is also shown in Figure 5C. The number of inactive contacts remained under 2 for the duration of the implant. The fluctuation in the number of excluded channels resulted mostly from a bad connection between the external connector and the amplifier and regained function during the recording sessions.
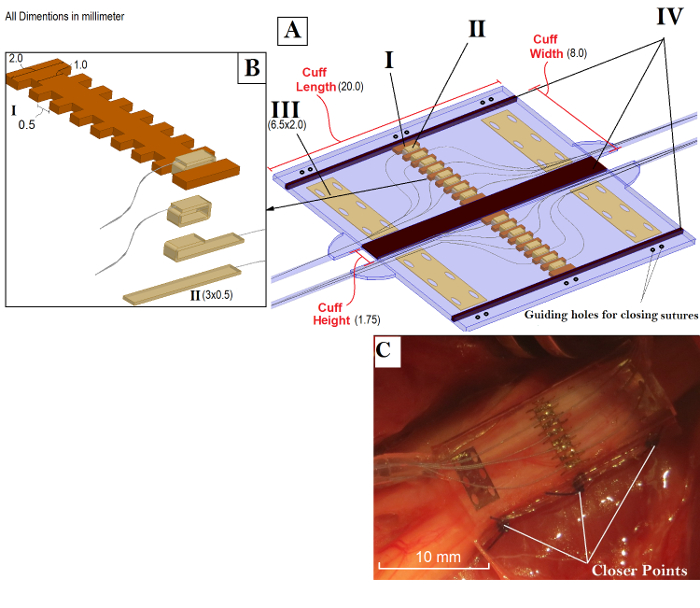
Figure 1: Overview of the FINE and its Components. A) FINE in the open position and the four main building components that require precision cut. These components are: Contacts array frame (I), the middle contacts strips (II), the reference contacts (III), PEEK spacers (IV). The cuff is facing downward with respect to the contacts placement against the nerve. The spacers (IV) are removed after the assembly. B) An expanded view of the center contacts and the steps to fold and fix them around the middle frame. C) Folded configuration of the electrode. Please click here to view a larger version of this figure.
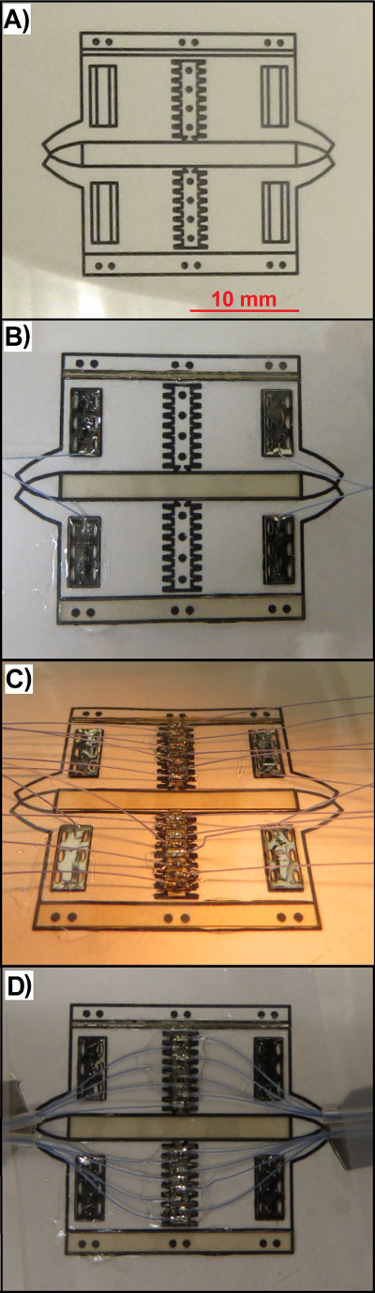
Figure 2: Snapshots of the Electrode during the Fabrication Process. A) The guiding diagram, T1 and S1 stacks at the end of step 4.1. B) Mounting the spacer segments and reference contacts at the end of step 4.7. C) Adhering the center contacts array to S1 sheet at the end of step 6.1. D) Arranging the leads and silicone tube before embedding them inside the electrode body at the end of step 6.5. Please click here to view a larger version of this figure.
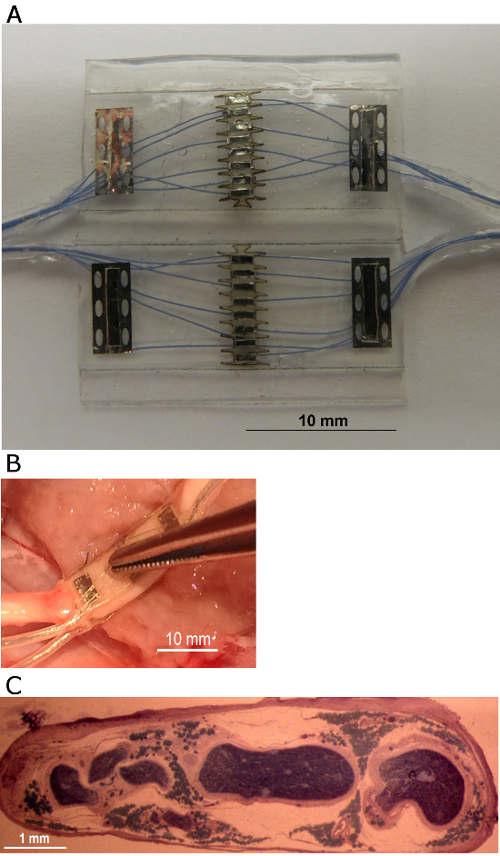
Figure 3: The Nerve Cuff Electrode Described in the Protocol. A) The fabricated 16 -contacts FINE in the open position. The leads are arranged into four bundles of 5 leads per exit site. B) An example of the placement of the cuff around the sciatic nerve in dog. The middle segment of the FINE remained flat in the transverse direction, and the cuff body is flexible in the longitudinal direction. C) A photograph of implanted nerve post mortem showing the flattened cross section and the arrangement of the fascicles after implanting a FINE electrode for 12 weeks. Please click here to view a larger version of this figure.
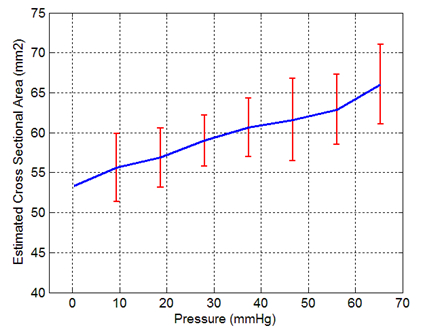
Figure 4: FINE Response to Increasing Internal Pressure. These measurements were made by placing an inflatable elastic chamber inside a closed cuff, and then the pressure was gradually increased by a variable -length water column. The major and minor axes of the cuff's cross section were measured at each pressure level and an elliptic cross section was assumed in order to calculate the cross sectional area (n= 20). The error bars represent the standard deviation.
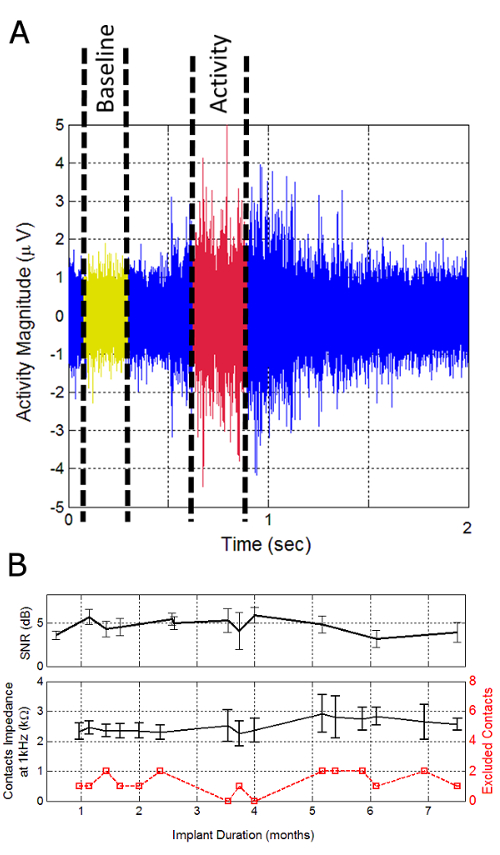
Figure 5: The Evaluation of Cuff Functionality with Chronic Recording of Sciatic Nerve Activity in Dogs. A) A Two seconds example of raw ENG signal recorded at one contact while the animal is voluntarily walking on a treadmill. SNR was defined as the ratio of activity and baseline mean powers. B) Average SNR values were observed during the implant duration. C) Mean value of contacts impedance at 1 kHz (black) and number of non-functional contacts over time (red). 14 of the 16 contacts remained functional throughout the implant duration. The error bars represent the standard deviation. Please click here to view a larger version of this figure.
