During the development of this model, multiple observations were made regarding factors that affect the duration of GBS vaginal colonization. To determine how estrous stage at inoculation impacts GBS bacterial persistence, mice were staged on the day of inoculation via vaginal lavage fluid. Figure 1 illustrates the four stages of the mouse estrous cycle, as determined by wet-mount vaginal lavage fluid, a well-established method29. Mice were divided into groups based on this initial stage, and GBS persistence was monitored over time via vaginal swabbing. Mice inoculated at the proestrus stage were colonized with GBS longer than any other stage of estrus, particularly those in diestrus at the time of inoculation (Figure 2). Based on these results, in the current model, mice are treated with β-estradiol one day prior to GBS inoculation to synchronize them into the proestrus stage.
Other murine models of reproductive tract infections have demonstrated an increased ability of the pathogenic organism to persist when mice are sustained in the estrus stage through exogenous estradiol treatment30,31. To determine if this phenomenon also occurred during vaginal colonization with GBS, GBS persistence was monitored during repeated β-estradiol treatment. Sustained estrus promoted GBS A909 (American Type Culture Collection, ATCC #BAA-1138) persistence in CD-1 mice, with 90% colonization 2 weeks post-inoculation (Figure 3A). In a typical experiment with one dose of β-estradiol prior to inoculation, only 40-50% of mice were colonized one week post-inoculation (Figure 4). The mean GBS CFU recovered from these mice mimics the percentage of colonization (Figure 3B). Although these results were obtained from independent experiments, these data demonstrate that maintaining continuous estrus promotes GBS vaginal persistence in the majority of CD-1 mice.
While conducting colonization experiments using different human GBS isolates, it was observed that strains varied in their ability to persist in CD-1 mice, ranging from several days to beyond a month. Of the strains tested, NCTC 10/84 had the shortest duration, A909 and COH1 persisted for one to two weeks, whereas strain CJB111 persisted in the majority of mice for two weeks (Figure 4) and even beyond a month (data not shown). To date, there has been no observed correlation of serotype and ability to persist in the mouse vaginal tract; however, significant differences between individual GBS strains have been reported25. The ability of GBS to colonize multiple inbred and outbred mouse lines was also examined. GBS strain A909 persisted in the vaginal tract for approximately one week in outbred CD-1 mice and inbred FVB mice (Figure 5). Alternatively, the majority of inbred BALB/c and C57BL/6 were colonized at one week (Figure 5) and remained colonized for a month or beyond (data not shown).
Using this protocol, GBS vaginal colonization in vivo was visualized by inoculating mice with a plasmid GFP-expressing GBS strain and collecting tissue for fluorescent microscopy. GFP-GBS was detected both adhering to murine vaginal epithelium (Figure 6A) and in close proximity to other native vaginal flora (Figure 6B). No GFP signal was detected in mice that had cleared the GFP-GBS at the time of tissue collection (data not shown).
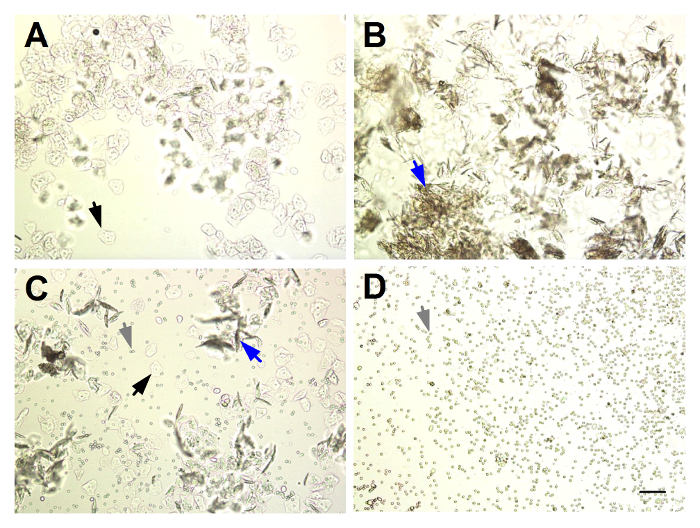
Figure 1: Identifying the Stage of Estrus from Unstained Murine Vaginal Lavage Fluid. (A) Proestrus: abundant nucleated squamous epithelial cells (black arrows). (B) Estrus: abundant cornified squamous epithelial cells (blue arrows). (C) Metestrus: mixture of nucleated and cornified squamous epithelial cells and predominantly leukocytes (grey arrows). (D) Diestrus: abundant leukocytes. Magnification = 100X, scale bar = 100 µm. Please click here to view a larger version of this figure.
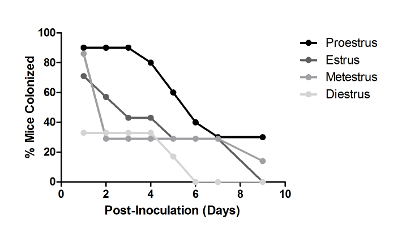
Figure 2: Estrous Stage Impacts Vaginal Persistence of GBS. Percent of CD-1 mice colonized with 1 × 107 CFU GBS A909 over time. Mice were grouped (n = 7 – 11/group) based on estrous stage at the time of GBS inoculation, as determined by vaginal lavage fluid. One independent experiment is shown. This figure has been modified from previously-published work and reprinted with permission19. Please click here to view a larger version of this figure.
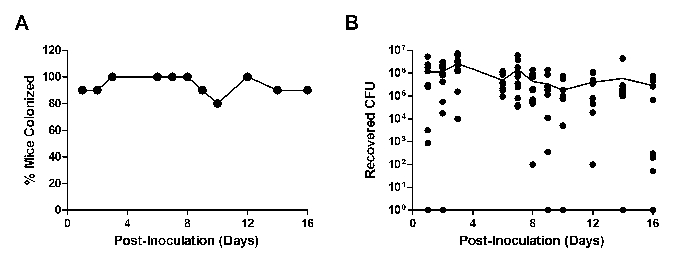
Figure 3: Continued Treatment with β-estradiol Promotes GBS Vaginal Persistence. Percent colonized (A) or recovered CFU (B) of CD-1 mice (n = 10) inoculated with 1 × 107 CFU GBS A909 and maintained on β-estradiol treatment. Mice were injected with β-estradiol one day prior to GBS inoculation and on days 1, 3, and 5 post-inoculation. One independent experiment is shown. The line in (B) represents mean recovered CFU. Please click here to view a larger version of this figure.
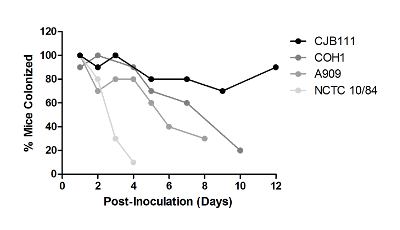
Figure 4: GBS Strains Differ in Their Ability to Persist in the Vaginal Tract. Outbred CD-1 mice (n = 10/group) were injected with a single dose of β-estradiol one day prior to GBS inoculation with 1 × 107 CFU of the given GBS strains. Experiments with each strain were carried out independently and were repeated at least three times; one representative result is shown. This figure has been modified from previously-published work and reprinted with permission25. Please click here to view a larger version of this figure.
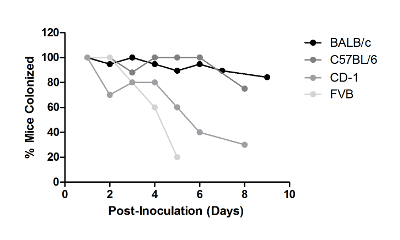
Figure 5: Mouse Strains Differ in Their Ability to Be Colonized with GBS in the Vaginal Tract. Mice from indicated background strains were injected with a single dose of β-estradiol one day prior to inoculation with 1 × 107 CFU of GBS A909. Experiments with each strain were carried out independently and were repeated at least twice; one representative result is shown. Please click here to view a larger version of this figure.
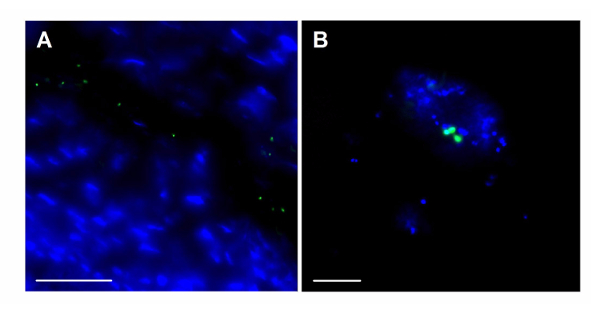
Figure 6: Fluorescent Imaging of GBS within the Mouse Vaginal Tract. Visualization of GFP- expressing GBS (green) along the vaginal epithelium at magnification = 630X, scale bar = 50 µm (A), and in close proximity to endogenous vaginal microbes at magnification = 1,000X, scale bar = 20 µm (B). Blue stain = DAPI. Please click here to view a larger version of this figure.
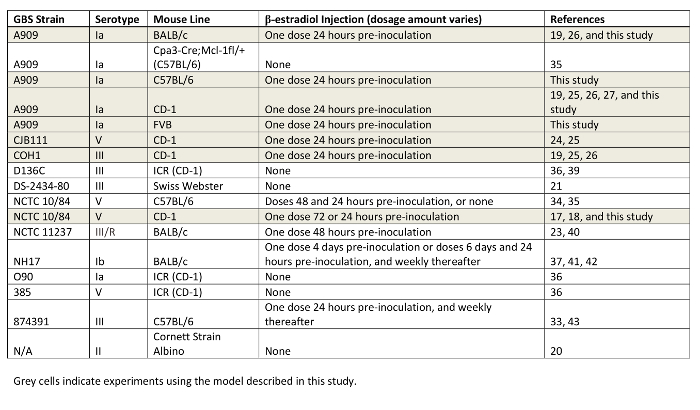
Table 1: Compilation of GBS Strains and Mouse Lines Utilized for Vaginal Colonization Studies. GBS background strains, mouse lines, and dosage of β-estradiol are indicated. Studies using the model described in this work are highlighted in grey.
