After centrifugation of anti-coagulated blood using a sucrose cushion, peripheral blood mononuclear cells (PBMCs) are enriched in an interphase on top of the density gradient medium (Figure 1). After the PBMCs are drawn off, FACS analysis is performed to characterize the different cell populations within the PBMCs using lineage markers (e.g., CD3 for T lymphocytes, CD14 for monocytes, and CD19 for B lymphocytes). Figure 2A shows the results of a representative FACS analysis of PBMCs collected and stained after density gradient centrifugation. Out of the gated population (Figure 2A, upper plot), we detected 4.03% B lymphocytes, 28.20% monocytes, and 67.62% other cells (Figure 2A, middle plot), of which 43.62% were T lymphocytes (Figure 2A, lower plot).
PBMCs are then incubated with CD14 magnetic particles and, following incubation on a magnet, the negative fraction containing the peripheral blood lymphocytes (PBLs) is analyzed by FACS using the selection of abovementioned lineage markers. Compared to PBMCs, we measured similar percentages of B lymphocytes (4.65%, Figure 2B, middle plot), higher percentages of other cells (88.61%, Figure 2B, middle plot), and strongly reduced percentages of monocytes (6.59%, Figure 2B, middle plot). Characterization of the positive fraction (Figure 3) demonstrated a high separation efficiency, since the purity of the isolated cells is over 97% (Figure 3, left plot), of which 99.56% (Figure 3, right plot) expressed high levels of CD14 on the cell surface.
IL4 and GM-CSF stimulation of monocytes for 5 days results in differentiation into monocyte-derived dendritic cells, which are comparable to dermal dendritic cells in morphology, behavior, and receptor expression19. FACS analysis of monocyte-derived dendritic cells on day 5 shows a homologous population (Figure 4, left plot) expressing high levels of CD11b, CD11c (not shown), and the C-type lectin DC-SIGN. No expression of the DC maturation marker CD83 is detected (Figure 4, right plot), and cells also lose the monocyte marker CD14 (not shown).
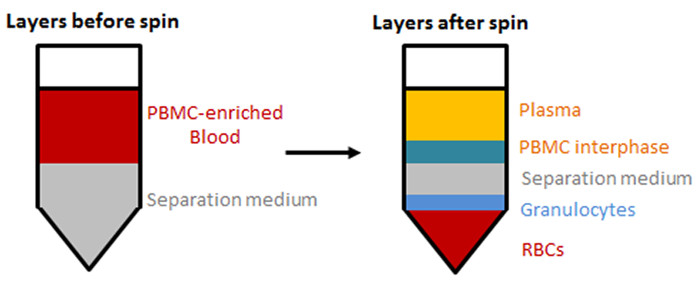
Figure 1: Separation of blood components by density gradient centrifugation. PBMCs are enriched in an interphase on top of the separation medium by density gradient centrifugation. Layers before (left) and after (right) centrifugation are shown. Please click here to view a larger version of this figure.
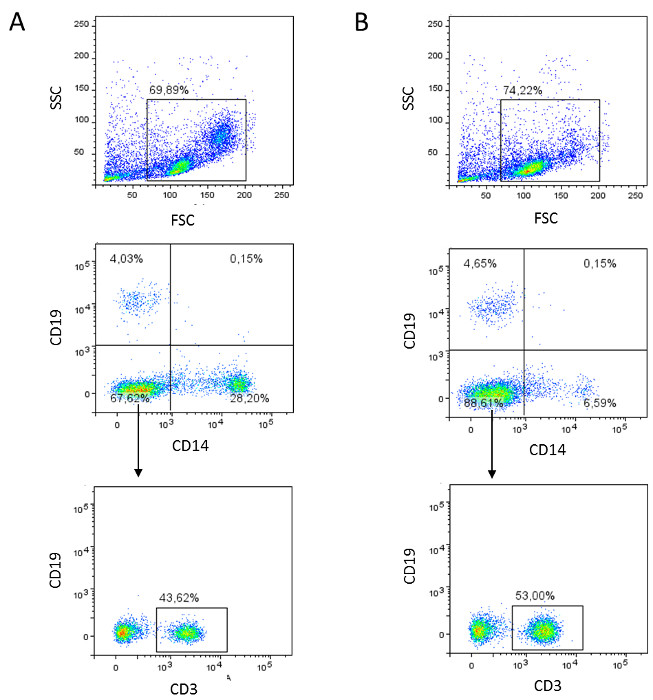
Figure 2: Flow cytometric analyses of PBMCs (A) and PBLs (B). (A) PBMCs are harvested, stained for lineage markers (mouse-anti-human CD3, CD14, and CD19 antibodies), and analyzed by flow cytometry. Dot plots of a representative result are shown. (B) The negative fraction containing PBLs is characterized by lineage markers (mouse-anti-human CD3, CD14, and CD19 antibodies) and analyzed by flow cytometry. Dot plots of a representative result are shown. Please click here to view a larger version of this figure.
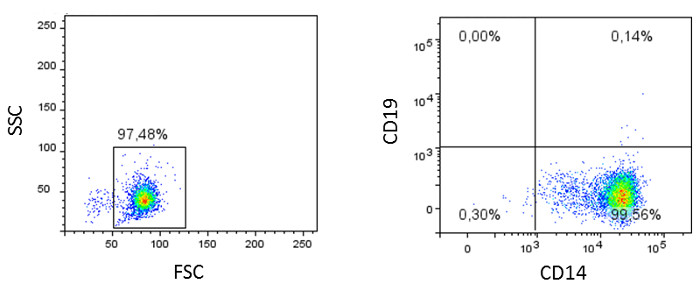
Figure 3: Flow cytometric analyses of monocytes. The isolated monocytes (positive fraction) are characterized using lineage markers (mouse-anti-human CD3, CD14, and CD19 antibodies) and analyzed by flow cytometry. Dot plots of a representative result are shown.
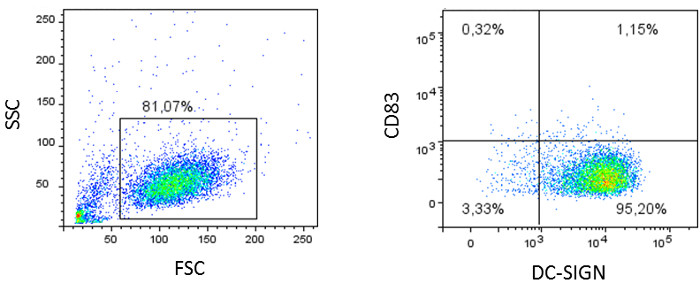
Figure 4: Flow cytometric analyses of monocyte-derived dendritic cells. Monocytes are stimulated for 5 days with IL4 and GM-CSF and stained for characteristic DC markers, like CD11b, CD11c (not shown), the C-type lectin DC-SIGN, and the maturation marker CD83. Dot plots of a representative result are shown.
