The manuscript describes an optimized protocol for the successful development of a xenograft mouse model for engraftment of MCL cells. Preparation of a pure cell population (in this case MCL cells), is very critical to develop successful MCL xenografts. Figure 1 represents the preparative steps for mononuclear cell isolation from MCL patient's blood by density gradient separation. The mononuclear cells are further processed to obtain pure B cells using a negative B cell enrichment kit to obtain a pure cell population for xenograft injection into mice. Care should be taken to obtain maximum purity in order to have successful MCL engraftment. The purity obtained using this method is usually >90%. The remaining cells were mainly monocytes and some T cells (data not shown).
Figure 2 represents the different steps of the B cell purification protocol as described in the methods section. The enriched cells are further analyzed for their purity by flow cytometer using different markers (CD45, CD19, CD20, CD23, CD200, CD5, kappa, and lambda). Sequential gating as shown in Figure 3 allows characterizing of MCL cells: CD45+, CD19+, CD20+, CD5+, CD23−, and CD200− are selected. Compensation for multicolor staining was carried out by using single stained controls for each of the fluorochromes used, according to standard cytometry set-up.
Figure 3E, G represents the typical dot plot of B cells before and after enrichment. In this case, >95% of the enriched cells using this kit are B cells. The cells are suspended in PBS at a concentration of 40 – 60 ×106 cells in 150 – 200 µL PBS as mentioned in the protocol. They were immediately injected i.v. to NSG mice. After 10 weeks, >90% of the injected animals developed lymphoma shows signs of terminal illness (weight loss, ruffled hair, decreased activity, etc.). After sacrifice, spleen and liver are removed and processed to obtain single cell suspensions by mechanical disruption (Figure 4D, F); blood is drawn carefully by cardiac heart puncture and the bone marrow is processed by cutting both ends of the femur and flushing it using a 2 mL syringe filled with RPMI medium or PBS (Figure 4C). The cells are further processed by flow cytometry using human B cell specific markers like CD19/CD20 and CD45. We used human B cell specific markers here because the recipient mouse strain (NSG) lacks B Cells. Figure 4B–F represents the collection of organs after sacrifice and the steps of further processing. The degree of engraftment of MCL cells derived from two patients is represented in Figure 4G. The engraftment pattern in different organs and between patients can be compared following this technique.
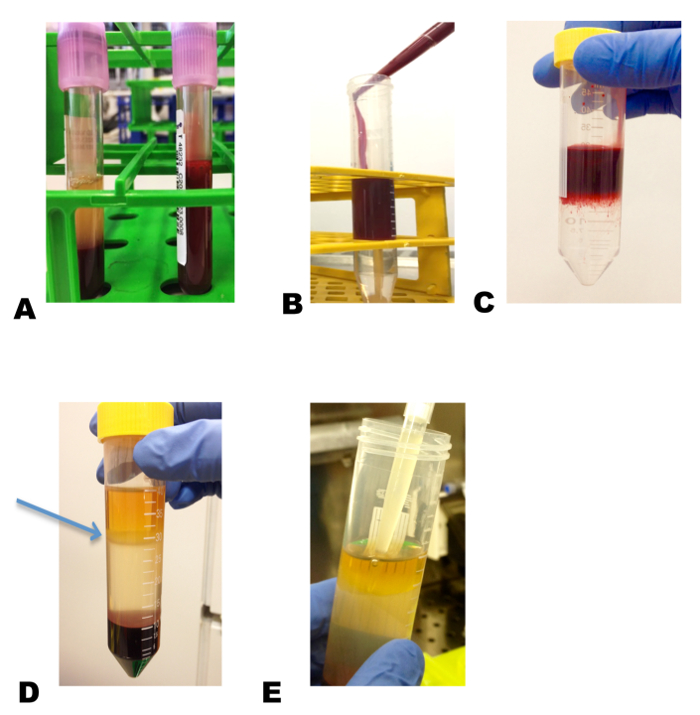
Figure 1: Isolation of PBMCs from whole blood. Blood drawn from a MCL patient is diluted 1:1 in RPMI medium (A), and placed carefully on top of the density gradient media layer (B) without mixing the blood into this density gradient media (C). Centrifugation at 400 x g for 45 min separates the mononuclear cells, which appear as whitish ring (arrow indicates the mononuclear cell layer) (D). This layer is pipetted gently without mixing with other layers into a clean tube for further processing (E). Please click here to view a larger version of this figure.
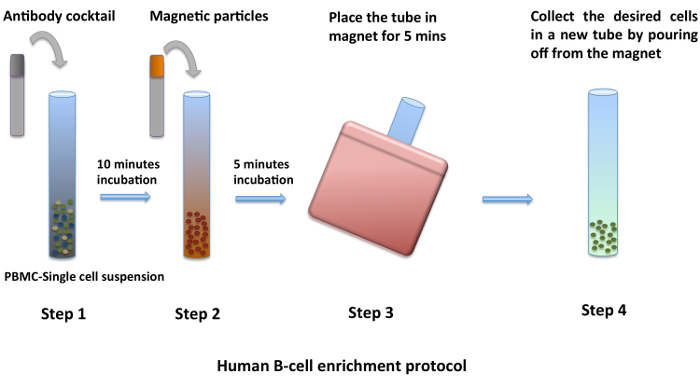
Figure 2: Enrichment of B cells from PBMCs. PBMCs isolated by density gradient centrifugation are washed twice with PBS. Using the negative B cell enrichment kit and by following the manufacturer's protocol, a pure population of B cells is obtained (1–4). Please click here to view a larger version of this figure.
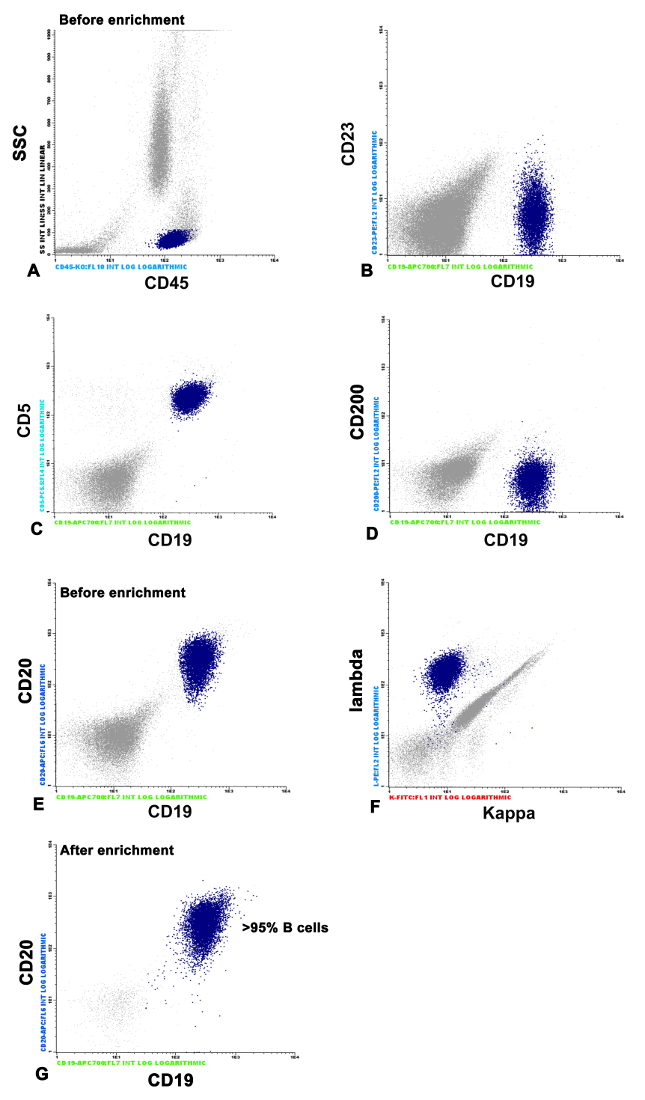
Figure 3: FACS analysis of MCL cells and purity of B cells before and after enrichment. The mononuclear MCL cells are characterized by FACS analysis using different markers like CD45, CD19, CD20, CD23, CD200, CD5, kappa, and lambda. Cells that are positive for CD45, CD19, CD20, CD5, and negative for CD23 and CD200 are selected (A–F). G represents the cell population after enrichment using the negative selection kit compared to E, which is before enrichment. Please click here to view a larger version of this figure.
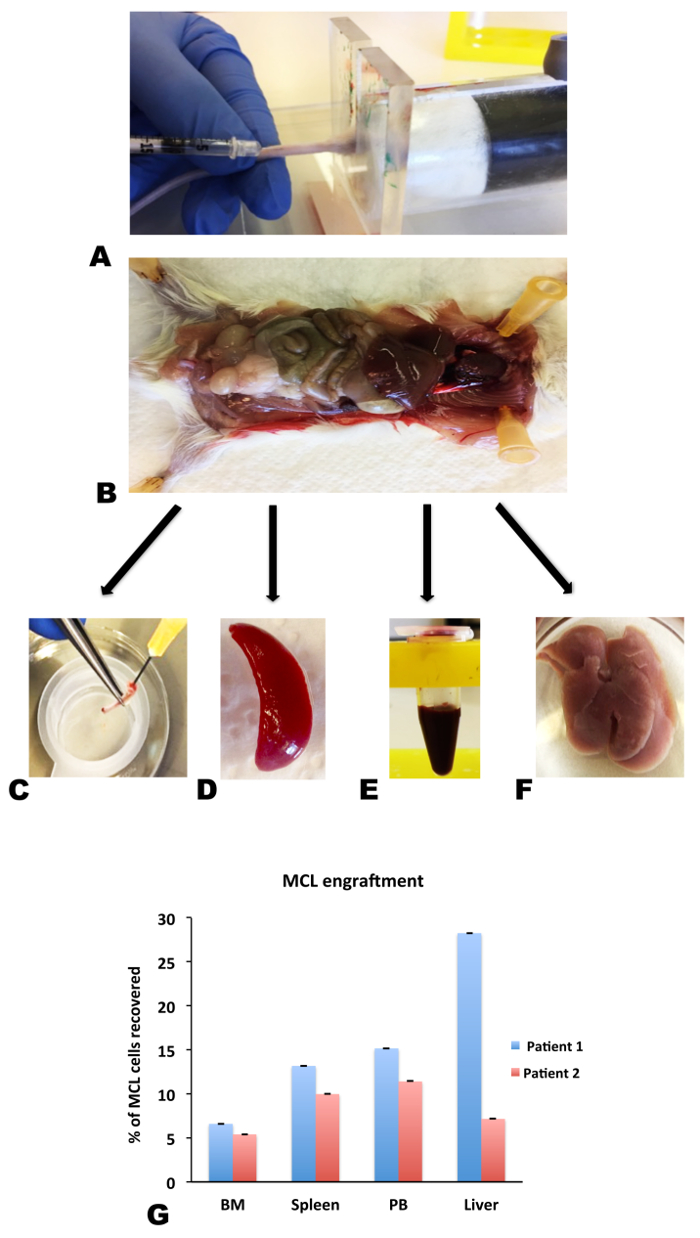
Figure 4: NSG mice as a xenograft model for engraftment of MCL cells. B cells derived from MCL patients were injected i.v. via the lateral tail vein of NSG mice (A). After allowing several days for the tumor to engraft, the mice were sacrificed, and dissected (B) to collect different organs like bone marrow (C), spleen (D), peripheral blood (E) (drawn by cardiac heart puncture), and liver (F). These organs were processed further and analyzed by flow cytometry for the presence of B cells. G represents the engraftment pattern of MCL cells in different organs derived from MCL injected NSG mice. Results from two patients are shown. Data are shown as mean ± SEM, n = 3. Please click here to view a larger version of this figure.
